Table of Contents
Cover
Title page
Copyright page
Dedication
Contributors
Foreword
Foreword
Foreword
Preface and Acknowledgments
Acknowledgments
1 The History of Joint Replacement in Veterinary Surgery
Total hip replacement
Total elbow replacement
Total knee replacement
Conclusion
2 Implant Materials: Structural
General metallurgy
Fabricating shapes
Adding porous coatings
Metals used for implant fabrication
Materials used in veterinary joint replacement systems
3 Implant Materials: Surface Coating
Surface treatment of cemented femoral stems
Surface treatment of cementless femoral stems and acetabular cup
Biologically active coatings
4 Weight-Bearing Surfaces
Polyethylene
Metal
Surface coatings
Ceramic
Articulations
5 Methods of Immediate Fixation
Introduction
Basic biomechanics and implant design
Cemented systems
Cementless systems
Combination: Hybrid fixation
Conclusion
6 Biomechanical Considerations in Total Hip Replacement
Functional anatomy of the hip joint
Mechanics of total hip replacement
Wear
Cemented implant interfaces
Cementless implant interfaces
Center of rotation
Version
Offset
Bearing diameter
Bearing type
Femoral head materials
Polyethylene
Design considerations of cemented femoral components
Design considerations of cementless acetabular components
Design considerations of cementless femoral components
7 Clinical Application of Total Hip Replacement
Introduction and background
Indications and contraindications
Preoperative planning
Surgical overview
Postoperative care and physical rehabilitation
Clinical outcomes and postoperative complications
Addendum: surgical procedures
8 Revision Strategies for Total Hip Replacement
Mechanical failure
Biological failure
General recommendations
9 Biomechanical Considerations in Total Knee Replacement
Gait analysis and kinematics of the stifle joint
Stifle joint loading
Mechanical versus anatomical axes
Role of ligaments
Stifle joint contact pressures
Design considerations for TKR implants
Mechanical factors at the femorotibial articulation
Mechanical factors at the implant–bone or cement–bone interface
Mechanical factors in periprosthetic tissues
Kinematics after TKR
Summary and conclusions
10 Clinical Application of Total Knee Replacement
Introduction
Historical perspectives
Indications for TKR
Preoperative considerations
Staging
Implant selection
Surgical procedure
Postoperative radiographs
Results
Complications
Future directions
11 Biomechanical Considerations in Total Elbow Development
History of total elbow replacements
Chapter overview
The elbow: Anatomy
Elbow biomechanics
Design principles of TER
Conclusions
12 Clinical Application of Total Elbow Replacement in Dogs
History of canine total elbow replacement
Evolution rationale of the ISU Elbow
Current systems: Design rationale summary
Indications and contraindications
Preoperative evaluation and planning
Surgical techniques
Postoperative evaluation and management
Clinical outcome: Complications
Needed and ongoing studies
Limitations of TER
Conclusions
13 Emerging Arthroplasties
Total disc arthroplasty
Shoulder arthroplasty
Arthroplasty of the carpus
Total ankle arthroplasty
14 Custom Total Joint Arthroplasty
The need for custom orthopedic implants
Fabrication of custom implants
Applications of custom implants
Index
This edition first published 2013 © 2013 by John Wiley & Sons, Inc.
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientific, Technical and Medical business with Blackwell Publishing.
Editorial offices: 2121 State Avenue, Ames, Iowa 50014-8300, USA
The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
9600 Garsington Road, Oxford, OX4 2DQ, UK
For details of our global editorial offices, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell.
Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by Blackwell Publishing, provided that the base fee is paid directly to the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923. For those organizations that have been granted a photocopy license by CCC, a separate system of payments has been arranged. The fee codes for users of the Transactional Reporting Service are ISBN-13: 978-0-4709-5961-9/2013.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
Library of Congress Cataloging-in-Publication Data
Advances in small animal total joint replacement / edited by Jeffrey N. Peck, Denis J. Marcellin-Little.
p. ; cm.
Includes bibliographical references and index.
ISBN 978-0-470-95961-9 (hardback : alk. paper) – ISBN 978-1-118-46271-3 (ePDF/eBook) – ISBN 978-1-118-46272-0 (ePub) – ISBN 978-1-118-46273-7 (eMobi)
I. Peck, Jeffrey N. II. Marcellin-Little, Denis J. (Denis Jacques), 1964–
[DNLM: 1. Arthroplasty, Replacement–veterinary. 2. Surgery, Veterinary–methods. 3. Pets–surgery. SF 911]
636.089′705–dc23
2012019773
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available in electronic books.
Cover design by Matt Kuhns
Disclaimer
The publisher and the author make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation warranties of fitness for a particular purpose. No warranty may be created or extended by sales or promotional materials. The advice and strategies contained herein may not be suitable for every situation. This work is sold with the understanding that the publisher is not engaged in rendering legal, accounting, or other professional services. If professional assistance is required, the services of a competent professional person should be sought. Neither the publisher nor the author shall be liable for damages arising herefrom. The fact that an organization or Website is referred to in this work as a citation and/or a potential source of further information does not mean that the author or the publisher endorses the information the organization or Website may provide or recommendations it may make. Further, readers should be aware that Internet Websites listed in this work may have changed or disappeared between when this work was written and when it is read.
Dedication
This book is dedicated to Kathy and Kayla, and to the memory of Cody Ruderman, who reminded me that our most serious complications should be our greatest impetus for advancement.
Jeffrey N. Peck
This book is dedicated to Terry, Arianne, and Julien, and to all loving owners of dogs and cats.
Denis J. Marcellin-Little
Contributors
Matthew Allen, Vet MB, PhD
Associate Professor
College of Veterinary Medicine
The Ohio State University
Columbus, OH
Michael Conzemius, DVM, PhD, Diplomate ACVS
Professor
College of Veterinary Medicine
University of Minnesota
St. Paul, MN
Loïc M. Déjardin, DVM, MS, Diplomate ACVS
Associate Professor
College of Veterinary Medicine
Michigan State University
East Lansing, MI
David J. DeYoung, DVM, Diplomate ACVS, ACVA
Adjunct Professor
College of Veterinary Medicine
North Carolina State University
Raleigh, NC
Reunan P. Guillou, Doc. Vet.
Assistant Professor
College of Veterinary Medicine
Michigan State University
East Lansing, MI
Ola L.A. Harrysson, PhD
Associate Professor
Fitts Department of Industrial and Systems Engineering
North Carolina State University
Raleigh, NC
Kei Hayashi, DVM, PhD, Diplomate ACVS
Associate Professor
College of Veterinary Medicine
University of California–Davis
Davis, CA
Michael P. Kowaleski, DVM, Diplomate ACVS, ECVS
Associate Professor
Cummings School of Veterinary Medicine
Tufts University
North Grafton, MA
William D. Liska, DVM, Diplomate ACVS
Surgeon
Gulf Coast Veterinary Specialists
Houston, TX
Kenneth Mann, PhD
Professor of Orthopedic Surgery
Director of the Musculoskeletal Science Research Center
Department of Orthopedic Surgery
Upstate Medical University
State University of New York
Syracuse, NY
Denis J. Marcellin-Little, DEDV, Diplomate ACVS, ECVS, ACVSMR
Professor
College of Veterinary Medicine
North Carolina State University
Raleigh, NC
Jeffrey N. Peck, DVM, Diplomate ACVS
Surgeon
Affiliated Veterinary Specialists
Maitland, FL
Melvyn Pond, BVMS, MRCVS, Diplomate ACVS
Surgeon
New Haven Hospital for Veterinary Medicine
Milford, CT
Mariana Quina, DVM
Surgical Resident
Affiliated Veterinary Specialists
Maitland, FL
Simon C. Roe, BVSc, PhD, Diplomate ACVS
Professor
College of Veterinary Medicine
North Carolina State University
Raleigh, NC
Kurt S. Schulz, DVM, MS, Diplomate ACVS
Surgeon
Peak Veterinary Referral Center
Williston, VT
Greg Van Der Meulen, BSME
Director of Research and Development
BioMedtrix, LLC
Boonton, NJ
Ketchum, ID
Foreword
The editors have asked me to write about my experience and thoughts on canine total hip replacements. I have often said that humans were the research animal for dogs when it came to total hip replacements. Although total hip replacements were being implanted in humans in the 1940s by surgeons such as Dr. Austin Moore, it was not until the late 1950s and early 1960s that Sir John Charnley’s work on implant design, materials, and fixation with polymethylmethacrylate (PMMA) bone cement made the procedure popular and widely used in humans. In 1957, Dr. Harry Gorman at The Ohio State University (OSU) worked on an experimental hip prosthesis in canines. These implants were cementless and the project was testing a design that was to be used humans. The femoral head was held in the acetabulum by a constraining metal ring, which was fixed to the pelvis with screws. This design was flawed and failed in most patients. However, Dr. Richard Rudy did tell me about one dog he implanted with this hip replacement that lasted for 13 years. It was not until 1974 when Dr. William Hoefle reported on a cemented total hip replacement in one dog that some people again began to think about doing this surgery in veterinary patients.
In early August 1976, 1 month after I started working at OSU, Dr. R. Bruce Hohn implanted the Veterinary College’s first Richards II Canine Cemented Total Hip Replacement. His second hip replacement occurred a few weeks later and I jumped at the chance to scrub with him on that hip. From that point on, we each did hip replacements at OSU. We wanted to document our technique, clinical results, postoperative care, and complications in a manner that would be most beneficial to the profession. Thus, we did not rush to publish our results but took time to reflect on what we learned. Our complication rate was high (20%) and by today’s standards would be unacceptable, but we found that as we accumulated cases and critically evaluated each complication, avoidable causes were identified. There was a marked reduction in complications in the last 2 years of this study. By continuing this evaluation even today, complication rates are minimized and now occur in approximately 7% of the cases.
Starting in 1977, an annual continuing education course was taught at OSU that included in the faculty both veterinarians and MDs from around the country who were implanting total hips. This gave valuable insight that was incorporated into the techniques used at OSU and around the world. These courses gave us an opportunity to exchange ideas and to teach the most current technique to veterinarians. It was not long before many veterinary surgeons were offering total hip replacements to their clients and patients.
When it became known that we were doing total hip replacements at OSU, there were those who said it was unnecessary to do this in dogs because excision arthroplasty (femoral head and neck ostectomy) worked well. We found that the easiest way for us to show the benefits of total hip replacement is to compare hip extended radiographs of a dog with a replaced hip and one with an excision arthroplasty taken 6 months after surgery. The total-hip dog will have well-developed muscle mass, while the excision-arthroplasty dog’s muscles are atrophied. The direct connection of the femoral head to the pelvis is important for the dog’s muscles and limb function to reach their full potential.
Our first major publication on the subject was a technique paper in a 1981 volume of Veterinary Surgery. The paper, documenting the results of the first 5 years of 221 consecutive clinical cases (216 of which had follow-ups for varying periods), did not come out until 1983. Since then, many more publications by myself and others have further expanded our understanding of canine total hip replacements. Total hip replacements have become a well-accepted technique for resolving discomfort and poor function resulting from canine hip diseases.
It became obvious to me as I worked with the Richards system that changes in implant design and instrumentation would be of benefit, so I discussed this with the company representatives. They declined to make changes. Thus, when in 1989 I was contacted about a new modular hip replacement system, I agreed to work on it. This collaboration resulted in the development of the BioMedtrix Canine Cemented Hip Replacement System. This company has been very receptive to changing the implants and instruments when clinical findings indicated that something was not working as well as it could, even if that was in just a few patients, or when a need was found that was not addressed by the system at a given time.
In an effort to improve what was offered to the patient, I was part of the group that worked on the cementless hip system for BioMedtrix. I saw the cemented and cementless systems as complementary to each other and felt they would expand the options a surgeon had available. I have not found one system to be overall superior to the other, but there are some cases where one system will work better for a given patient. In some cases, they can even be combined into a hybrid hip replacement. The surgeon who wants to provide the best possible service to the client and patient will be well versed in all aspects of both the cemented and cementless total hip replacement systems.
In human medicine, total hip replacement is considered the most consistently reproducible surgery with the most predictable results. This should also be true in veterinary medicine. It takes strict attention to detail, technique, and patient selection and care. The success rate of 95% dogs returning to normal to near-normal function is found no matter which implant is used. It is up to the surgeon to choose the best implants for a given patient.
Marvin L. Olmstead, DVM, MS
Emeritus Professor, The Ohio State University
Emeritus Diplomate, American College of Veterinary Surgeons
Surgeon, Oregon Veterinary Referral Associates
Foreword
This textbook constitutes a summary of the current stage of arthroplasty in veterinary surgery. The foreword written by Marvin Olmstead provides us with a historical perspective of the landmark work of the pioneers of arthroplasty in veterinary medicine over the last quarter of the twentieth century. Not only was the technique developed by these individuals, but they also pushed arthroplasty beyond the barriers of the time and made total hip replacement the treatment of choice for veterinarians, as well as pet owners. It is important for the next generation of orthopedic surgeons to be aware of the steps that got us to this point and shoulder the responsibility of advancing the science and art of arthroplasty in the future.
As veterinary orthopedic surgeons, we have the responsibility to critically assess implant and patient performance and continue to develop implants and techniques to improve the outcomes for our patients. The ultimate goal of total joint replacement is to relieve pain, improve the patient’s quality of life by returning function, and improve the client’s relationship with their pet. In addition, the prosthesis should last the lifetime of the patient. Success toward meeting these goals has been measured using a variety of standards, most often retrospective studies involving assessment of patient function, as well as client satisfaction.
While clinical assessment is the most important outcome assessment, and was paramount to achieving improvements during the early stages of cemented total hip replacement in dogs, additional advancement could only be achieved using more finite criteria for implant performance. It was clear that patient function did not always correlate with radiographic assessment. In the mid-1980s, a retrieval analysis program was started at North Carolina State University (NCSU), offering us the opportunity to assess cemented implants, and the surrounding cement and bone harvested following the death of canine patients. The program provided the opportunity to assess mechanical stability of the implant–cement and cement–bone interfaces, establish the nature of the cells in fibrous membranes, and search for the presence of particulate debris. Serial sectioning of femurs with intact implants and cement revealed cement cracks or an incomplete cement mantle that provided channels for wear debris to gain access to the cement–bone interface leading to osteolysis. Over a period of years, serial radiographic assessment and retrieval analysis pointed out many of the failure mechanisms associated with bone cement and cementing techniques. These were addressed with varying degrees of success in dogs over the past decade. Every attempt has been made to link failures back to patient selection and surgical technique, and in some cases implant materials or design. Critical assessment of failures is the most direct path to improving implant longevity. However, to call them failures while the dog is running and jumping may not be appropriate; perhaps it is best to use the term “early indicators of impending problems.” Changes leading to loss of implant stability are generally slow and insidious. They may take years, or in some cases, they may transpire at a frighteningly fast rate. In addition to clinical performance, serial radiographic assessment is the best clinical evidence of the implant performance over time and helps the surgeon reconstruct the causes of the failure. The important fact is to recognize the mechanisms of failure and take steps to minimize them or prevent them from occurring in future cases.
In 1986, an opportunity presented itself from David Hungerford, an orthopedic surgeon at Johns Hopkins University. He proposed to develop a cementless total hip system for clinical and research use in dogs in conjunction with surgeons at NCSU. The vision was to create a state-of–the-art cementless total hip system complete with accurate instrumentation. The system was to be used in research animals as well as clinical patients and to be implanted by the same team of veterinary surgeons. Having surgeons familiar with the hip system, implantation technique, performance, and assessment would enhance the quality of the research arm of the program. The same standards would be used for clinical and research animals and serial radiographic assessment would be used throughout the clinical and research studies, as well as retrieval analysis. This was the critical step that resulted in the development of the Canine PCA Total Hip System by Howmedica Inc. Multiple research studies were completed over a 15-year period, including a long-term prospective clinical trial. Research projects included the study of a variety of implant types and surface coatings and provided the team with extensive knowledge and experience that was applied to clinical patients. In retrospect, one significant decision was the training and use of an independent and unbiased observer to read all radiographic assessments made on the research studies, as well as clinical patients. A member of our team, Rick Schiller, was responsible for the reading, documentation, and interpretation of the radiographic studies for all research and clinical animals. Many of the research studies were subsequently reviewed by a third-party consultant, Tom Gruen. The extensive clinical and research experience gained using the Canine PCA Total Hip System laid the foundation for the development of the BioMedtrix BFX Cementless Total Hip System nearly 20 years later. Concurrently, others had evolved an interest in cementless fixation leading to the development of the Zurich Cementless Total Hip Replacement System in the 1990s by Pierre Montavon and Slobodan Tepic in Zurich, Switzerland. Multicenter clinical studies were led by Randy Boudrieau in the United States and Aldo Vezzoni in Europe.
Another critical initiative in the advancement of canine hip arthroplasty was the initiation of a series of conferences, “Contemporary Issues in Canine Total Joint Replacement,” held in 1999, 2000, 2001, 2005, and 2008. This conference was established with the goal to advance the science and art of canine total joint replacement. The objectives were to promote open discussion and debate on issues in total joint replacement using a variety of implant systems, actively engage surgeons and engineers in dialogue, emphasize optimal surgical technique for primary and revision arthroplasty procedures, and provide a forum for all participating surgeons to share their personal experiences. Significant changes were achieved as a result of the participation and contribution of surgeons attending these interactive conferences.
The first conference focused on the indications for hip replacement, patient selection, patient care, and surgical technique of cemented implants. The second conference in 2000 concentrated on surgical technique including canal and acetabular preparation, implant positioning and complications, revisions, and radiographic assessment. The 2001 conference expanded to include the clinical experience using a variety of cemented and cementless implants from the United States as well as Europe, including the CFX, PCA, Zurich Cementless, and the Biomécanique implant systems. This meeting proved to be a pivotal moment for cementless applications. The presentations on the clinical experience with the Zurich Cementless and the Canine PCA stimulated intense discussions and revealed how much interest there was in the positive results of cementless implants, and the desire to move in that direction was established. The next conference was not held until 2005, 2 years following the release of the BFX system. The entire meeting was dedicated entirely on the BFX cementless system, refinement of the operative technique, and resolving early complications. The last conference held in 2008 focused on refining the CFX and BFX operative procedures and instrumentation into a single system, the Universal Hip System. Input was provided by surgeons based on their experiences with the system over the past 3 years. These discussions led to the later refinement of the operative technique into a common Universal technique for CFX and BFX systems. Key observations and input from surgeons including Teresa Schiller, Denis Marcellin-Little, Loïc Déjardin, Melvin Pond, Michael Kowaleski, and Bill Liska were instrumental in refining the surgical technique, resulting in a reduction of early surgical complications. This conference also for the first time expanded to include micro hip implants and total knee and total elbow replacement. The 3-year gap between 2005 and 2008 was a very productive time for the advancement of total joint replacement in dogs.
It is my hope that this textbook will not only provide a valuable reference source for surgeons, but remind them just how far we have come in a relatively short time and excite them about the possibilities for the future. Through continued critical assessment including basic research and prospective clinical studies, we will continue to make strides to achieve our goal. The format of interactive conferences to share ideas and experience is also critical in achieving consensus and direction.
David J. DeYoung, DVM, Diplomate ACVS, ACVA
Professor Emeritus, Orthopedic Surgery, College of Veterinary Medicine,
North Carolina State University
Dean Emeritus, School of Veterinary Medicine, Ross University
Foreword
The American College of Veterinary Surgeons (ACVS) Foundation is excited to present Advances in Small Animal Total Joint Replacement in the book series entitled Advances in Veterinary Surgery. The ACVS Foundation is an independently charted philanthropic organization devoted to advancing the charitable, educational, and scientific goals of the American College of Veterinary Surgeons. Founded in 1965, the ACVS sets the standards for the specialty of veterinary surgery. The ACVS, which is approved by the American Veterinary Medical Association, administers the board certification process for Diplomates in veterinary surgery and advances veterinary surgery and education. One of the principal goals of the ACVS Foundation is to foster the advancement of the art and science of veterinary surgery. The Foundation achieves these goals by supporting investigations in the diagnosis and treatment of surgical diseases; increasing educational opportunities for surgeons, surgical residents, and veterinary practitioners; improving surgical training of residents and veterinary students; and bettering animal patients’ care, treatment, and welfare. This collaboration with Wiley-Blackwell will benefit all who are interested in veterinary surgery by presenting the latest evidence-based information on a particular surgical topic.
Advances in Small Animal Total Joint Replacement is edited by Drs. Jeffrey N. Peck and Denis J. Marcellin-Little, both Diplomates of the American College of Veterinary Surgeons and prominent small animal orthopedic surgeons in the field of total joint replacement. They have assembled the leaders in the field of joint replacement, presenting a historical perspective of joint replacement in veterinary surgery, the relevant issues regarding implant materials, the common sites of total joint replacement, including the hip, knee, and elbow, emerging arthroplasties sites, and the use of custom prostheses. The ACVS Foundation is proud to partner with Wiley-Blackwell in this important series and is honored to present this book in the series.
Mark D. Markel
Chair, Board of Trustees
ACVS Foundation
Preface and Acknowledgments
Joint replacement for companion animals has been available for approximately four decades. Fortunately, over time, several pioneers have pushed the boundaries of our knowledge, technology, and capabilities. Several of these early pioneers, such as Hap Paul, Dave Nunamaker, and Tom Turner, were veterinarians who embraced the “One Medicine” philosophy and were involved in the early development of both human and veterinary joint prostheses.
Until the 1990s, joint replacement in veterinary surgery had mostly been limited to the hip and was available at only a small number of institutions. As we grew to expand the breadth of joint replacements available to our patients, we have been enduring the same growing pains and made errors similar to our human surgeon counterparts. Most often, we start out by creating highly constrained prostheses with restricted kinematic function. As our understanding of the kinematics and biomechanics of the normal joint grows, so does the likelihood of repeatable, successful long-term outcomes.
In addition to expanding the armamentarium of available joint replacements, there has also been a substantial increase in the number of surgeons performing joint replacement procedures worldwide. In order to maximize the success of any new procedure, it is critical that the surgeon’s knowledge and skill exceed what is necessary to simply perform the procedure. A deeper level of understanding is necessary to minimize the incidence of complications and to manage them when they occur. Furthermore, a larger population of knowledgeable surgeons will accelerate the rate at which we can improve on existing designs and procedures.
This book’s aim is to facilitate the advancement of joint replacement in veterinary surgery by pooling the existing body of information and providing a solid foundation of knowledge to joint replacement surgeons. That knowledge is necessary to provide optimal patient care, to conduct clinical research, and to educate future surgeons.
Acknowledgments
We thank all implant manufacturers for their support. We thank Terry Marcellin-Little for her assistance with the Index, and Dr. William D. Liska for the radiograph used on the cover.
Jeffrey N. Peck
Denis J. Marcellin-Little
1
The History of Joint Replacement in Veterinary Surgery
Mariana Quina and Jeffrey N. Peck
Total joint replacement has gained an important place in veterinary orthopedic surgery. There are currently commercially available prosthetic components and instrumentation for canine and feline total hip replacement, canine total elbow replacement, and canine total knee replacement. Although many different implant systems have been developed for experimental use, descriptions of the implants in this chapter are limited to the commercially available systems.
Total Hip Replacement
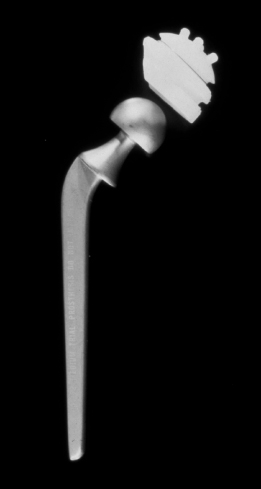
Total hip replacement became commercially available in the dog in 1974 (Hoefle 1974). The implant system used was a cemented, fixed-head, stainless steel femoral component and polyethylene acetabular cup that was available in three sizes (Richards Manufacturing, Memphis, TN; Figure 1.1). The Richards II canine total hip prosthesis was the only commercially available canine system until 1990. Design modifications to the implants were made in the late 1970s in order to decrease the tendency for luxation, provide more consistent placement of the acetabular component, and reduce the possibility of damage to the femoral component during preparation of the femur. These changes included a 20-degree cutaway on the dorsal aspect of the acetabular component, establishment of a guide system for placement of the acetabular component, several minor changes to the femoral component design, and introduction of a femoral component trial prosthesis to be used during preparation of the femur.
In 1979, Leighton reported on the use of the Richards II system in nine experimental dogs. Each of the three available sizes of prostheses was implanted in three dogs each. Of the nine dogs, there was one failure due to infection resulting in acetabular component loosening. The remaining eight dogs reportedly had good or excellent function 1 year after surgery. Use of the Richards II system was reported in a clinical setting with good success (Lewis and Jones 1980; Olmstead et al. 1983). Lewis and Jones performed 20 total hip replacements in 15 dogs and reported the results with a minimum of 1-year follow-up. The most common complication was loosening of the acetabular component, the femoral component, or both. Causes of aseptic loosening were not clearly identified or understood at the time of the Lewis publication. Contributing factors to implant loosening that were identified included infection, inadequate preparation of the bone prior to cement placement, undersizing of implants, and improper positioning of the implants. Other complications included failure of the femoral component via bending or breakage at the stem–neck angle and luxation. Only six of the hips did not have postoperative complications. Four of the 20 hips were eventually explanted. Of the remaining 16, 75% were considered to have excellent outcome.
Olmstead et al. (1983) reviewed 221 total hip replacements over a 5-year period. Follow-up information was available for 216 of the cases. The minimum follow-up period for inclusion in the study was 4 weeks, and of the 149 hips that were not lost to follow-up at study completion, none had an evaluation period shorter than 25 weeks. At the final evaluation, 91% were reported to have satisfactory function, with owners reporting increased activity levels, improved muscle mass, and elimination of pain. Of the dogs with bilateral hip dysplasia, unilateral hip replacement resulted in enough improvement in clinical signs that surgery on the contralateral side was not deemed necessary for 80% of dogs. Complications included luxation, infection, aseptic loosening of the acetabular component, femoral fracture, and sciatic neurapraxia. The overall complication rate was 20%, with 58% of cases with complications eventually achieving a satisfactory outcome. Evaluation of follow-up radiographs, as well as what constituted a satisfactory outcome, was not discussed.
In June 1990, the BioMedtrix CFX® system (BioMedtrix, Boonton, NJ), a modular cemented total hip prosthesis and instrumentation set, was introduced (Olmstead 1995). The most significant change in this modular system compared with the fixed-head system was the introduction of a two-piece femoral component. The femoral component consists of a stem and a head secured together via a locking taper mechanism. This change allowed for three different neck lengths for each stem. The original CFX femoral stem was made of titanium alloy (TiAlVn) and was available in five sizes. The head was made of cobalt-chrome and available in three sizes. New instrumentation was also introduced, including power reaming of the femur and acetabulum to increase accuracy and the ease of the procedure. Olmstead (1995) reported preliminary clinical results for 52 total hip replacements using this system. Follow-up ranged from 2 months to 15 months (mean: 6 months) and consisted of owner questionnaires regarding the dogs’ function following total hip replacement. Only two complications were reported, one luxation and one iatrogenic intrapelvic hematoma causing urethral compression, both of which were resolved successfully with additional surgical intervention. In 2004, Liska reported on 730 consecutive hip replacements using the BioMedtrix CFX system, with a mean follow-up of 3.9 years.1 Complications included both craniodorsal and ventral luxation, infection, aseptic loosening, femur fracture, sciatic neuropraxia, pulmonary embolism, incision granuloma, extraosseous cement granuloma, medullary infarction, and osteosarcoma. The procedure was considered successful in 96% of cases. The Liska study included the most comprehensive description of outcome and complications to date. While several of these complications had been described in case reports (Roe et al. 1996; Marcellin-Little et al. 1999a,b; Sebestyen et al. 2000; Bergh et al. 2006), this large study was the most comprehensive to date and it allowed a direct comparison of the rate of all complications. The BioMedtrix CFX system is discussed in detail in Chapter 7.
The original total hip replacement femoral implants were made of stainless steel. Newer generations of femoral implants were made of titanium alloy. Titanium is resistant to corrosion and is highly biocompatible, making it an attractive material for surgical implants. However, under certain conditions, particularly when used as a cemented stem, titanium alloys are more susceptible to severe abrasive corrosive wear than stainless steel or cobalt-chrome alloys (Agins et al. 1988). This is primarily associated with the elastic modulus mismatch between cement and titanium and the proclivity of titanium alloys to generate wear debris under such condition (see Chapters 3 and 6). Lee et al. (1992) found an unusually large amount of metal debris in the tissues around titanium alloy prostheses showing early failure as well as larger polyethylene particles in tissues from failed titanium alloy than from cobalt-chrome or stainless steel prostheses. These particles lead to wear debris, which stimulates macrophage recruitment and cytokine release and result in bone resorption and, therefore, aseptic loosening (Goldring et al. 1983).
Uncemented total hip replacement techniques have been developed to avoid the use of cement, which, despite improvements in cementing techniques, continues to be implicated in irreversible infections and aseptic loosening (DeYoung et al. 1992; Marcellin-Little et al. 1999b). Skurla et al. (2005) investigated aseptic loosening in 38 total hip replacements from 29 client-owned dogs. The duration of implantation ranged from 8 months to over 11 years and all were postmortem retrieval specimens. Nine of the femoral components were grossly loose and 15 were mechanically loose, for a total of 63.2% loose implants. Stem loosening occurred more commonly at the cement–implant interface than at the cement–bone interface. No significant difference was found in loosening rates for implants retrieved in the short term (defined as less than 3 years) and in the long term. Edwards et al. (1997) also reviewed aseptic loosening in 11 total hip replacements in 10 dogs. Loosening of the femoral component occurred at the cement–implant interface at a mean of 30 months postoperatively. Radiographic changes associated with aseptic loosening included asymmetrical periosteal reaction along the femoral diaphysis, radiolucent zone at the stem–cement interface, altered implant position, and femur fracture. They found that aseptic loosening was significantly more common when the distal tip of the femoral component was in contact with the cortical endosteum than when there was no contact.
The clinical use of the PCA Canine Total Hip system (Howmedica, Mahwah, NJ) was reported, but was not commercially produced for the veterinary market (DeYoung et al. 1992; Marcellin-Little et al. 1999a). However, the PCA system is considered the predecessor for the BioMedtrix BFX® system. DeYoung et al. (1992) described the PCA implant design as well as the surgical technique for implantation. The femoral component of this system was available in four sizes, each made of cast cobalt-chromium alloy with porous coating at the proximal one-third of the stem. The modular femoral head allowed for two different femoral neck lengths and to be used interchangeably with the stems and acetabular components. The acetabular component was a cast cobalt-chromium alloy with a backing of three layers of beads and an ultrahigh-molecular-weight polyethylene insert. Two polyethylene insert depths were also available. Both the acetabular and femoral components were a press-fit with long-term stability imparted by porous bone ingrowth. A preliminary study was done on 60 experimental hips followed by 40 clinically affected hips in 32 client-owned dogs. The overall success rate for the 100 total hips was 98%. There were six complications including three luxations, two fissure fractures of the femur, and one displacement of the acetabular component due to improper positioning. Only two of the hips were eventually explanted. Marcellin-Little et al. (1999b) reported on 50 consecutive total hip replacements in 41 dogs. Mean long-term follow-up was 63 months. Radiographically, all cups and stems had bone ingrowth fixation and no evidence of osteolysis, late stem subsidence, or cup tilting. At the long-term follow-up, 74% of hips had normal function. Of those with abnormal function, three had luxations and the remainder had unrelated problems causing abnormal hind limb gait.
The Zurich Cementless Total Hip Replacement system (Kyon, Zurich, Switzerland) has been available since the late 1990s (Guerrero and Montavon 2009). In this system, the femoral components are made of titanium and titanium alloy and the acetabular component is lined with ultrahigh-molecular-weight polyethylene. The femoral stem in this system is anchored to the medial cortex of the femur with locking screws. This design is intended to decrease complications resulting from subsidence, as well as micromotion at the bone–implant interface. Stress shielding of the bone is also meant to be minimized.2 This prosthesis is discussed in detail in Chapter 7. The BioMedtrix BFX system is an uncemented total hip replacement system designed to be interchangeable with the BioMedtrix CFX system. It was commercially introduced in 2003. The femoral and acetabular components of the BFX system are press-fit and designed to allow porous ingrowth for long-term stability. This prosthesis is discussed in detail in Chapter 7.
The dog has been used as a model for human total hip replacement for decades. Total hip replacement in the dog as a model for the development of a prosthesis for human use was first reported in 1957 (Gorman 1957). Gorman implanted a cementless, stainless steel prosthesis in over 50 dogs. The acetabular component was stabilized using three toggle bolts and the femoral component was simply inserted into the femoral canal without fixation, although the first-generation stem was transfixed to the medullary canal (Figure 1.2). The femoral head was retained within the acetabular component by a retaining rim to prevent luxation. The author reported generally positive results.
Chen et al. (1983) performed total hip replacement in 13 dogs. The cementless femoral component was square in cross section and with a titanium core and a 2-mm outer layer of unalloyed 50% fiber titanium composite. Seven dogs were implanted with a cementless acetabular component of ultrahigh-molecular-weight polyethylene and a cylindrical outer surface, coated with unalloyed titanium fiber. The remaining six dogs were implanted with cemented acetabular components. Bone ingrowth occurred in all porous-coated implants; however, no mechanical testing was performed in this study to evaluate the strength characteristics of the implants. All of the animals walked without functional deficits and all femoral stems and acetabular cups were stable at 6 months postoperatively.
Gitelis et al. (1982) studied the effects of weight bearing on the bone–cement interface in cemented total hip replacements in two groups of six dogs. A cobalt-chrome femoral component and ultrahigh–molecular-weight polyethylene acetabular component were implanted using acrylic cement. In one group, immediate weight bearing with unrestricted activity was allowed, while in the second group amputation distal to the knee was performed in order to prevent weight bearing. Three of the dogs in the weight-bearing group had postoperative luxation. These dogs were eliminated from the study and replaced with three new dogs. Endosteal bone remodeling with a fibrous membrane located between the endosteal surface of the bone and cement was found in both weight-bearing and nonweight-bearing dogs. The study found that early postoperative weight bearing was not a factor in bone remodeling at the bone–cement interface and surrounding bone.
Dowd et al. (1995) investigated the role of implant motion, titanium alloy, cobalt-chrome alloy, and polyethylene particles in the process of osteolysis and aseptic loosening. Forty dogs had total hip replacements and were assigned to the control group or one of five experimental groups. The control group had a standard prosthesis implanted. The prosthesis was modified for the experimental groups to create a motion model, a gap model, and three particulate debris models (a titanium model, a cobalt-chrome model, and a high-density polyethylene model). Two dogs had intraoperative femur fracture during implantation and were excluded from the study. One dog had a postoperative luxation, underwent open reduction, and remained in the study. All dogs had a clinically normal gait by 2 weeks after surgery. After 12 weeks, the femurs were harvested. All control implants were stable with no obvious motion between the implant and bone. All of the experimental implants had some degree of motion and the femoral prosthesis was easily separated from the femur. Histological and biochemical assessment of the periprosthetic tissues from the control group had relatively acellular periprosthetic tissue with low levels of biochemical activity. In contrast, assessment of the motion group as well as all three particulate debris groups showed increased numbers of macrophages as well as increased levels of biochemical mediators of bone resorption consistent with osteolysis.
Among the most interesting uses of the canine model for human total hip replacement was the use of Robodoc, an industrial robot adapted for used in surgery (Paul et al. 1992). The purpose of this study was to determine whether robotic preparation of the femoral canal would result in improved implant–bone contact and fewer intraoperative cracks or fissures compared to hand broaching for a cementless total hip prosthesis. The clinical portion of this study included 25 canine patients with robotic femoral canal preparation and 15 patients with manual femoral canal preparation. Robotic preparation resulted in a higher implant–bone contact than manual preparation and resulted in no fissures or cracks.
Total Elbow Replacement
The first clinical case of total elbow replacement in small animals was reported in 1964 (Whittick et al. 1964). A custom-manufactured, hinged, constrained stainless steel prosthesis was implanted in a cat with comminuted fractures of the distal humerus and proximal radius and ulna. Due to inherent constraints of the implant design the cat had limited range of motion of the elbow postoperatively, but the results were considered acceptable. Three months postoperatively, the cat was estimated to use its leg at 80% of normal function and was able to resume its normal activities, including running and climbing trees.
Unlike total hip replacement and total knee replacement, there is no comparable human model for elbow osteoarthritis in dogs. In addition, the elbow presents the additional challenge of being a three-bone joint, with the inherent risks this poses to implant loosening. Nevertheless, the high incidence of end-stage elbow osteoarthritis in dogs with relatively few treatment options has encouraged several groups to work toward total or partial elbow (unicompartmental) replacement.
Since the late 1990s, a constrained hinged system, a four-component nonconstrained system, and a semiconstrained system have been designed, tested, and abandoned prior to publishing any results due to high complication rates (see Chapters 11 and 12; Conzemius 2009). The TATE Total Elbow (BioMedtrix) consists of a preassembled, prealigned combined humeral and radioulnar implant. Preliminary trials using the TATE Total Elbow were reported by Acker and Van Der Meulen in 2008. The system was implanted in six client-owned dogs with elbow pain secondary to end-stage osteoarthritis.3 Complications included an epicondylar fracture with pin migration, ulnar nerve transection, and implant malpositioning with a humeral crack. At the time of the report, none of the dogs had required explantation. The TATE prosthesis is discussed in detail in Chapter 12.
The BioMedtrix (Iowa State) Canine Elbow has been used clinically for more than 10 years. Conzemius and colleagues initially reported on its use in six normal dogs in 1998 and again in 2001. The 1998 prototype system was a cemented snap-fit semiconstrained system that yielded suboptimal results, with loosening of the radioulnar component in five of six dogs (Conzemius and Aper 1998). The system was modified to an unconstrained, cemented, two-component system consisting of a stainless steel humeral component and an ultrahigh-molecular-weight polyethylene radioulnar component (Conzemius et al. 2001). Three of six dogs in the later report had excellent results, with normal use of the operated limb 1 year after surgery (Conzemius 2009). Modifications to the BioMedtrix elbow were made based on these results, and the system was implanted in 20 client-owned dogs with severe radiographic elbow osteoarthritis and daily lameness from elbow pain unresponsive to medical management (Conzemius et al. 2003). The revised system was still an unconstrained, cemented, two-component system made from the same materials as previously. This system and its current (third-generation) design are described in detail in Chapter 12.
Total Knee Replacement