Contents
Contributors
Preface
General Aspects of Trauma
CHAPTER 1 General Principles: How to Interpret Radiographs
Rules of two
Ten commandments
ABCs systematic assessment
Further reading
CHAPTER 2 Hand
Anatomy
ABCs systematic assessment
Injuries
CHAPTER 3 Wrist
Anatomy
ABCs systematic assessment
Injuries
CHAPTER 4 Elbow
Anatomy
ABCs systematic assessment
Other injuries
Other information
ABCs systematic assessment – summary
Further reading
CHAPTER 5 Shoulder
Anatomy
ABCs systematic assessment
Injuries
CHAPTER 6 Pelvis and Hip
Anatomy
ABCs systematic assessment
Pelvis
Hip
Femoral neck fractures
Acetabular fractures
Dislocation
Congenital dislocation of the hip
Idiopathic coxa vara
Slipped capital femoral epiphysis (adolescent coxa vara)
CHAPTER 7 Knee
Anatomy
ABCs systematic assessment
Injuries
CHAPTER 8 Ankle
Anatomy
Radiographic projections
ABCs systematic assessment
Mechanisms of injury
CHAPTER 9 Foot
Anatomy
ABCs systematic assessment
Calcaneal injuries
CHAPTER 10 Chest
Anatomy
ABCs systematic assessment
Systematic review of the lungs
Trauma related conditions
Some non-trauma related conditions
CHAPTER 11 Abdomen
Anatomy
ABCs systematic assessment
Common abdominal emergencies
Gastrointestinal emergencies
Others
CHAPTER 12 Head
CT technique
ABCDEF systematic assessment – primary assessment of cranial CT
Key areas for review
Head injuries
Primary brain injury
Meningitis
Subarachnoid haemorrhage
Stroke
Vascular territory infarct
Intraparenchymal haemorrhage
Hypertensive haemorrhage
CHAPTER 13 Face
Anatomy
ABCs systematic assessment
CHAPTER 14 Cervical Spine
Anatomy
ABCs systematic assessment
Interpretation of lateral radiographs
Interpretation of anteroposterior radiographs
Interpretation of open mouth odontoid radiographs
Pitfalls
Physiological mimics of injury in children
CHAPTER 15 Thoracic and Lumbar Spine
Clinical examination
Anatomy
ABCs systematic assessment
Injuries
CHAPTER 16 Emergency Paediatric Radiology
Fractures
Anatomy
Types of fracture
Physeal fractures
Elbow injuries
Forearm fractures
Painful hips
Non-accidental injury
Chest emergencies
Acute abdominal emergencies
Renal tract emergencies
Further reading
CHAPTER 17 Major Trauma
Primary survey
Adjuncts to primary survey and resuscitation
Interpreting primary survey images
Index
© Blackwell Publishing Ltd 2007
BMJ Books is an imprint of the BMJ Publishing Group, used under licence
Blackwell Publishing Inc., 350 Main Street, Malden, Massachusetts 02148-5020, USA
Blackwell Publishing Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UK
Blackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton, Victoria 3053, Australia
The right of the Author to be identified as the Author of the Work has been asserted in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording and/or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior written permission of the publisher.
First edition 1995
Second edition 2007
1 2007
Library of Congress Cataloging-in-Publication Data
ABC of emergency radiology. -- 2nd ed. / edited by Otto Chan.
p. ; cm.
Includes bibliographical references and index.
ISBN-13: 978-0-7279-1528-3
ISBN-10: 0-7279-1528-2
1. Radiography, Medical. 2. Emergency medicine--Diagnosis. I. Chan, Otto.
[DNLM: 1. Radiography. 2. Emergencies. WN 200 A134 2007]
RC78.A562 2007
616.07’572--dc22
2006103167
ISBN: 978-0-7279-1528-3
A catalogue record for this book is available from the British Library
The cover shows avulsion of the anterior cruciate ligament and is used with permission of Otto Chan
Set in 9.25/12 pt Minion by Sparks, Oxford – www.sparks.co.uk
Printed and bound at GraphyCems, Navarra, Spain
Commissioning Editor: Mary Banks
Editorial Assistant: Victoria Pittman
Development Editor: Sally Carter / Vicki Donald
Production Controller: Rachel Edwards
For further information on Blackwell Publishing, visit our website: www.blackwellpublishing.com
The publisher’s policy is to use permanent paper from mills that operate a sustainable forestry policy, and which has been manufactured from pulp processed using acid-free and elementary chlorine-free practices. Furthermore, the publisher ensures that the text paper and cover board used have met acceptable environmental accreditation standards.
Blackwell Publishing makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check that any product mentioned in this publication is used in accordance with the prescribing information prepared by the manufacturers. The author and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this book.
Contributors
Consultant Musculoskeletal Radiologist, Barts and The Royal London NHS Trust, London
Ultrasound Consultant, Addenbrooke’s Hospital, Cambridge
Consultant Radiologist, Stoke Mandeville Hospital, Buckinghamshire
Consultant Radiologist, The London Independent Hospital, London
Consultant Radiologist, Radiology Red Dot Courses, London
Consultant in Paediatric Radiology, Great Ormond Street Hospital, London
Consultant Radiologist, King’s College Hospital, London
Specialist Registrar in Diagnostic Radiology, King’s College Hospital, London
Consultant Interventional Radiologist, The Royal London Hospital, London
Consultant Maxillofacial Surgeon, The Royal London Hospital, London
Associate Professor of Radiology, University of California San Diego, USA
Consultant Paediatric Radiologist, Royal London Hospital, London
Lecturer, University of Athens, Athens, Greece
Consultant Radiologist, Royal Bournemouth Hospital, Bournemouth
Consultant Neuroradiologist, Charing Cross Hospital, London
Assistant Professor of Radiology, Mount Sinai Hospital and University Health Network, University of Toronto, Toronto, Canada
Hôpital Lariboisière, Paris, France
Consultant Radiologist, Royal London Hospital, London
Formerly Consultant Radiologist, University College Hospital London
Professor, University of Arizona Health Sciences Center, Tucson, Arizona, USA
Specialist Registrar in Diagnostic Radiology, King’s College Hospital, London
Professor, Department of Diagnostic Radiology, University of Maryland School of Medicine, Baltimore, USA
Assistant Professor, University of Maryland Medical School, Baltimore, USA
Consultant Radiologist, Nuffield Orthopaedic Centre, Oxford
Consultant in Emergency Medicine, St Mary’s Hospital, London
Consultant Trauma and Vascular Surgeon, The Royal London Hospital, London
Consultant in Accident and Emergency, The Royal London Hospital, London
Specialist Registrar in Radiology, Barts and The Royal London NHS Trust, London
DISC Imaging, Mount Pleasant SC United States
Preface
There have been dramatic technological advances in diagnostic imaging over the past two decades, but the rapid acquisition and interpretation of plain radiographic images remains the mainstay of initial successful management of sick or traumatised patients in accident and emergency departments.
Virtually any medical condition can present to accident and emergency departments, and so the volume of medical knowledge needed to manage these patients satisfactorily is enormous. It is unfortunate that most of these patients are initially seen and treated by relatively inexperienced staff – usually medical students, house officers, senior house officers, specialist registrars, or nurses – who often have had little or no training in the interpretation of plain radiographs.
Rapid and accurate interpretation of these radiographs is often the key to quick and correct management of patients in the accident and emergency department. Although safety nets exist, specialist radiological advice is often not available at the time of presentation – when it is most needed. Staff in the accident and emergency department who manage these patients need to be able to interpret these radiographs for quick, accurate, and effective initial treatment, to avoid errors in interpretation, inappropriate treatment, and medicolegal consequences.
The authors of the ABC of Emergency Radiology have produced a simple and logical step by step approach on how to interpret radiographs. The book is divided into anatomical regions and followed by chapters in paediatrics and major trauma. The chapters start with normal basic radiological anatomy, followed by the standard radiographs, then a simple ABCs systematic approach on basic interpretation of the radiographs, a review of abnormalities, and a summary.
This book provides a simple, concise, and systematic approach to the interpretation of plain radiographs. It should be very helpful to medical students, foundation doctors, specialist registrars, and consultants in all specialties, and also other health professionals working in accident and emergency, in particular radiographers and nurses.
Otto Chan
To my family.
Trauma was long regarded as a subject unworthy of study and research in medicine. The serious collective morbidity and mortality caused by trauma has now been acknowledged, and the enormous collective costs of the initial treatment and subsequent care have been computed and tabulated. The numbers are large. As a result, trauma is now a matter of conscious concern to the medical profession and government at all levels. Trauma is finally receiving the attention it deserves.
In 1966, publication of the landmark white paper, Accidental death and disability, the neglected disease of modern society, by the National Academy of Sciences showed the full impact of trauma. It resulted in dramatic changes. Guidelines were published to establish regionalised trauma care, and they have been adopted widely in the United States. Anderson and colleagues carried out a similar study in the United Kingdom, and this has led to a sea change in the management of trauma in the United Kingdom. The introduction of advanced trauma life support training has been of great importance. Where adopted and implemented, specialised trauma centres have substantially improved the care of the injured. The need for research into trauma is vital because of its effect on the quality of life of people who have sustained trauma injuries and because of the high cost of treatment (more than $20 billion a year in the United States alone).
Trauma can occur to anyone at any time. Skeletal injuries occur during the course of all human activities. The expectation and risk of injury varies with the nature of the endeavour. Nobody is immune, irrespective of age, sex, activity, or state of health. Trauma is un expected and sudden. At best, an injury may cause a minor degree of inconvenience; at worst, it can cause death. Before the event, those affected may have been in excellent health. In the next moment, life may hang precariously in the balance. Of course, criminal activities, assaults, and beatings result in skeletal injury, but no human activity is free of the risk of injury. Even mundane activities in the home, at work, or at play carry a finite risk.
Repetitive activities in industrial settings lend themselves to analysis, and preventive measures can be taken to reduce the incidence of injury. In other situations, effective preventive measures have been identified, but they have been only partially accepted by the public. Laws have long been in place that set speed limits, prohibit driving while under the influence of alcohol, and mandate the use seat belts, yet many people ignore these laws and are a menace to themselves and others.
Injuries and death associated with motor vehicle crashes at high speed have reached plague-like proportions. With permission from Peter Menzel/Science Photo Library.

The location, nature, and number of fractures depend on the age of the individual, the nature and severity of the trauma, and the status of the skeletal system.
The activity in which a person is engaged when injured can be predicated by their age. The young will probably be injured in the course of play or sports activities. Mature adults (aged 20-50 years) are more likely to sustain an injury while travelling in a motor vehicle or at work. Falls are more often a source of injury in elderly people than other causes, including motor vehicle crashes. Many elderly people are sedentary, often affected by osteoporosis, and more likely to be injured in a fall during the course of normal activities – for example, walking, descending stairs, stepping from a curb, or moving about in a bathroom.
In the developed world, injuries are the leading cause of death for more than half of the human life span (1-43 years). Trauma is the fourth most common cause of death after heart disease, cancer, and stroke. About 150 000 US citizens of all ages die from trauma each year, and about a third of these deaths are from motor vehicle crashes. Motor vehicle crashes are the leading cause of death between the ages of 5 and 34 years.
The World Health Organization (WHO) has estimated that in the year 2000, 1.26 million people worldwide died from road traffic crashes. Injuries outnumber all other causes of death in children and young adults. Almost half of all deaths in US children are the result of trauma. Crashes involving motor cars and children who are pedestrians are the leading source of multiple injuries in children. Such incidents are followed distantly by motor vehicle crashes with children as passengers, crashes involving children on bicycles and motor vehicle crashes involving motor cycles, and falls from great heights. Children tend to survive multiple injuries more often than adults.
The overall death rate of those who sustain multiple injuries is about 10-25%. People >70 years are affected more severely by accidents than those from other age groups. Trauma is the fifth leading cause of death in patients >65 years. Although people in this age group are less likely to be injured than those in younger age groups, older individuals are more likely to die from their injuries. In older people, mortality from accidents is five times higher than that in younger people.
The first two steps in the care of an injured person should be a carefully performed medical history and physical examination. An evaluation of the airway and checks for the presence of shock, haemorrhage, and open wounds are essential. In each of these areas, corrective measures must be taken immediately if necessary. Fractures should be noted and splints applied. These actions will assist in the handling of the patient and reduce morbidity in seriously injured patients.
The portion of the average life span during which injuries are the main cause of death in the United States. Adapted from Baker SP. Injuries: The neglected epidemic. Stone Lecture1985. American Trauma Society Meeting. J Trauma 1987;27:343.

Death rates in the United States for injuries by age, 1930-1980. Adapted from Baker S P. Injuries: The neglected epidemic. Stone Lecture 1985. American Trauma Society Meeting. J Trauma 1987;27:343

The physical examination of comatose patients or patients with multiple injuries (often seen in patients from vehicle accidents) is difficult because the patient is unable to cooperate or respond to queries. Injuries can be easily overlooked, which heightens the importance of imaging.
Radiographic examination should never be considered a substitute for taking a patient’s history and doing a physical examination. Serious injuries can often exist even if they are not found on a radiograph.
Successful treatment of skeletal injury starts with accurate diagnosis. A good history and physical examination, and to ensure the patient is haemodynamically stable is necessary for this. Then the patient needs a well performed and accurately interpreted radiographic examination. The standard views for radiographs have been adopted because they show most abnormalities. Failing to obtain all of the standard views heightens the chance for oversights and diagnostic errors.
A radiographic examination to exclude a skeletal injury of any anatomical part should never be obtained in a single plane only. Radiographs obtained in two planes at right angles are the minimum, and radiographic examinations of joints need additional oblique views to exclude fractures and dislocations. Patients who have severe trauma require computed tomography to identify or exclude injuries of the central nervous system, vascular area, chest, and intra-abdominal visceral injuries, as well as injuries of the face skeleton, spine, and pelvis.
The physician or radiologist’s interpretation of a radiographic examination (or any type of imaging examination) is facilitated greatly by an appropriate history on the request form. Unfortunately, the history being included for the radiologist can be perfunctory, incomplete, or even misleading. The lack of a good history compromises the radiologist’s evaluation. The history should state precisely where the patient hurts and the initial clinical impression – for example, “Pain in snuff box, rule out fracture of the scaphoid.” Knowledge of where the patient hurts directs attention to the area of principal clinical concern and, at the same time, steers the radiologist away from questionable findings in other parts of the film that have no clinical importance.
Injuries are repetitive. That is to say, in each anatomical part injuries occur at some sites more often than at others. People who interpret radiographs of patients with trauma should be aware of the sites of the most common injuries in each anatomical part. They should exclude injuries at those specific sites. For example, with pain in the wrist – epiphyseal fractures of the distal radius should be excluded in adolescents, scaphoid and triquetral fractures are most common in young adults, and Colles’ fractures should be looked for in elderly people.
In a patient’s history, a simple anatomical diagram that shows where the patient hurts, clearly marked in pen or pencil by the doctor, is extremely helpful. This figure is adapted from a patient assessment form for use by staff working in fast response vehicles.

Soft tissue signs that point to underlying injury of the bone and joint should be specifically identified or excluded. These include the fat pad sign at the elbow joint, which indicates haemoarthrosis, and the fat-fluid sign at the knee, which alerts the doctor to an intra-articular fracture of the knee joint.
Emergency medicine often brings together critically ill patients with inexperienced junior doctors – a dangerous combination with potentially serious consequences. The huge volume of information necessary to manage these patients adequately is overwhelming, as virtually any condition can present itself. The difficulties are compounded because radiographs are requested for many patients. These radiographs may be interpreted by relatively inexperienced, and often tired, personnel who have little training in how to evaluate them.
Radiographic projections
| Site | View | Comment |
| Finger | Anteroposterior and lateral | |
| Hand | Anteroposterior and oblique | |
| Wrist | Anteroposterior and lateral | Four views for suspected scaphoid fractures |
| Elbow | Anteroposterior and lateral | Additional views if fat pad present |
| Shoulder | Anteroposterior and Y view | |
| Pelvis and sacrum | Anteroposterior only | Coccyx views rarely indicated |
| Hip | Anteroposterior and oblique | Anteroposterior of both hips and oblique or lateral of injured hip |
| Knee | Anteroposterior and lateral | Lateral is done with a horizontal beam |
| Ankle | Anteroposterior and lateral | Anteroposterior mortice view for trauma |
| Feet and toes | Anteroposterior and oblique | |
| Cervical spine | Anteroposterior, lateral, and peg | Lateral must show C7/T1 (otherwise computed tomography) |
| Thoracic spine and | Anteroposterior and lateral | |
| lumbar spine | ||
| Chest | Posteroanterior erect or anteroposterior | Also anteroposterior supine (trauma) |
| Abdomen | Anteroposterior supine | Erect anteroposterior chest radiograph helpful |
| Head | Computed tomography scan | Plain skull radiographs rarely indicated |
| Face | Occipitomental and occipitomental 30° | Posteroanterior or posteroanterior 20° |
| Mandible | Anteroposterior view and orthopantomograph | Oblique view if orthopantomograph not available |
| Foreign bodies | Anteroposterior and lateral or tangential | Metal marker at entry site. Consider ultrasonography first or computed tomography |
The rules of two are a simple set of guidelines. Most rules should be obvious and some relate to specific problems, but they are useful general principles that help to avoid errors in interpretation of radiographs and management of patients.
Preferably, the two views should be perpendicular to each other. This rule applies to virtually all radiographs obtained, except for those of the chest, abdomen, and pelvis. Rarely, the abnormality is not visible at all or is subtle on the first view.
Rule 1 Anteroposterior (left) and lateral view of right ankle (right). The anteroposterior view was considered normal. The lateral view shows a displaced oblique fibula fracture (arrows).

Image the joint above and below a long bone. This particularly relates to mid-shaft injuries of the forearm (radius and ulna) and lower leg (tibia and fibula). Sometimes subtle injuries may be present in the joint above or below the obvious fracture.
Rule 2 Anteroposterior view of right leg (left), lateral view of right knee (middle), and anteroposterior view of right knee (right). Shows a Salter-Harris type II injury – proximal tibial metaphysis is fractured, with separation and displacement of the epiphyseal growth plate and undisplaced fibula fracture (arrowhead).

Rarely, the abnormality may be difficult to detect, and comparison with the other side can be helpful, especially in children. Always get a second opinion before requesting another radiograph because it means exposing the patient to additional radiation (an especially important consideration with children).
Rule 3 Anteroposterior view of right elbow (left) and anteroposterior view of left elbow (right). The right elbow has a non-united, avulsed, right medial epicondyle (arrow). The injury is obvious when compared with the normal left elbow with fused epiphyses.

Do not stop looking after you find one abnormality. An underlying predisposing cause may be the reason for the fracture (pathological fracture), or an unrelated incidental finding (such as a “bone island”) might be present.
Rule 4 Anteroposterior view of right humerus shows pathological fracture through lytic metastasis (arrow).

Rule 5 Septic arthritis in big toe. Initial film (left) was considered normal, but the loss of the joint space and the rapid progression confirms the diagnosis. The radiograph in the middle was taken when the diagnosis was made. The radiograph on the left was taken two weeks before, and the radiograph on the right was taken two weeks after the diagnosis.

If old films are available, always take the oppor tunity to look at them. This is particularly relevant in chest radiographs, because previous films will tell you if the latest radiograph shows an old or new find-ing. Similarly, if there is a bony abnormality, in particular if osteomyelitis or a septic arthritis is suspected, old films are essential for early diagnosis.
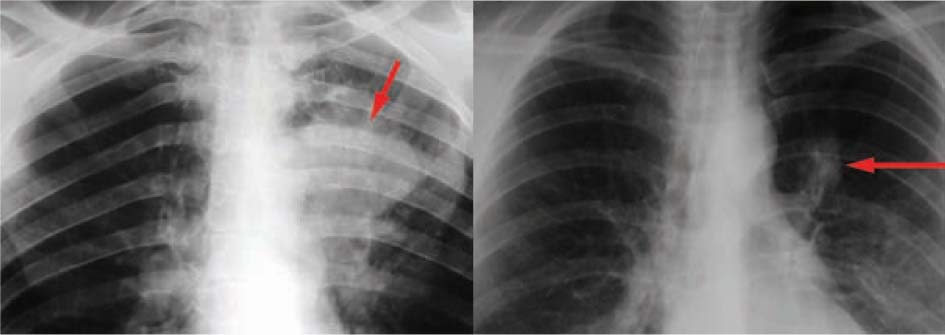
Rule 5 Posteroanterior chest radiograph (magnified view). Shows a primary bronchogenic carcinoma. Comparison with the chest radiograph of the same patient that was taken a year earlier (right) shows that the left hilar mass has enlarged over a year. The posteroanterior chest radiograph on the right (magnified view) was thought to be normal, but in retrospect, the tumour was visible (arrow).
Always bring the patient back for a repeat set of radiographs after a procedure – especially after surgery, setting a fracture in plaster, reducing a dislocation, or removing a foreign body.
Sometimes the patient should come back for a repeat film after a set period of time to see whether the abnormality has resolved, got worse, or not changed. Classic scenarios in which this would be appropriate include a suspected scaphoid fracture or when abnormalities on chest radiographs are seen and an old film is not available for comparison.
Rule 6 Lateral view of elbow in a plaster of Paris. Mid-shaft ulna is fractured (arrowhead), but the dislocated radial head had not been reduced (arrow).

Wherever possible, get a second opinion or show the radiograph to someone else. This is especially important if you are unsure about the radiograph. If the red dot system is used in your hospital, then this can be your first opinion.
The red dot system was introduced to help emergency department doctors. It is a voluntary system where the radiographer who took the radiograph gives his or her opinion as to whether the film is abnormal by placing a red dot next to the abnormality. It was initially, and in most hospitals still is, used for the peripheral skeleton only – that is, limb injuries. The red dot system helps to reduce errors and improve accuracy.
Radiographers are usually extremely experienced at taking films, looking at and interpreting them. Always ask the radiographer who took the film for their opinion first, especially if there is a red dot and you cannot find an abnormality.
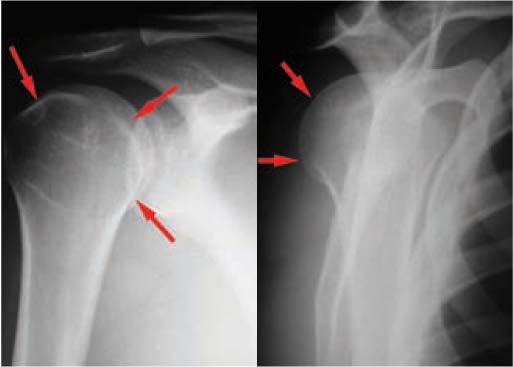
Rule 7 Anteroposterior view (left) and Y view (right) of right shoulder shows subtle posterior dislocation of the shoulder (arrow). Initially, these radiographs were interpreted as normal. The patient was then recalled to the emergency department by the radiologist for clinical review.
Apart from recording the history and results of the examination, always record the findings of the radiograph. It is easy to look at the film and to forget to write down the findings. Films get lost, and your written record may be the only record.
All films should be seen and reported formally by a radiologist. This is particularly important for films that are at first thought to be normal because the patient is usually discharged and may not be seen by anyone else.
Sometimes, if the plain radiograph is normal, the symptoms may warrant further investigation. Studies have shown that if a scaphoid fracture is suspected and the scaphoid series of films are normal, the patient should have a magnetic resonance image scan when possible, rather than putting the patient in a splint or plaster and waiting 10–14 days before taking another set of films, which is “accepted normal management.”
In addition, several abnormalities detected on plain radiographs warrant further imaging. If a fracture extends to the major joints (for example, acetabular and tibial plateau fractures), a computed tomography scan of the joint should be done routinely to evaluate the extent of joint involvement and to exclude loose fragments.
Rule 10 Anteroposterior view of scaphoid (left) and T1 weighted coronal magnetic resonance image (right) showing scaphoid fracture. Scaphoid series normal, but magnetic resonance image shows a fracture (arrow).

Touquet’s ten commandments are a simple set of guidelines to protect staff and hospitals from the inevitable mistakes that inexperienced doctors will make. Unfortunately, the commandments are often ignored. Many of the ten commandments are incorporated in the rules of two.
Certain conditions or injuries should be treated on the basis of the clinical findings initially, especially if the injury is life threatening (such as a tension pneumothorax). With other injuries, delaying initial treatment to obtain a radiograph is unnecessary (for example, a dislocated ankle). The delay may be either life threatening, or have long term sequelae. In addition, a finding on the radiograph may be an incidental finding (the fourth rule in the rules of two).
Command 1 Left tension haemopneumothorax. The patient should have been treated with a chest drain insertion before the chest radiograph was taken.

Command 1 Dislocated left ankle. The ankle should have been reduced without the radiograph.

A thorough clinical history and examination enables the mechanism of injury to be established, and the appropriate radiographs can then be requested. Knowledge of the mechanism of injury can often help to determine the likely pattern of injuries.
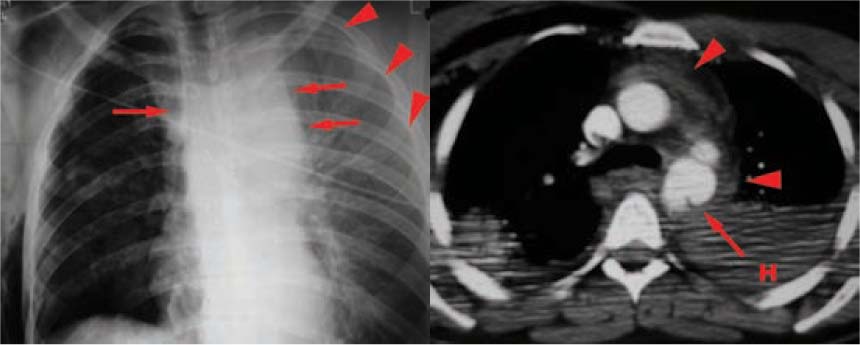
Command 2 Chest radiograph taken after a road crash (left) showing a widened mediastinum (arrow), and a haemothorax (arrowhead). A traumatic aortic injury was suspected and a computed tomogram was requested. The computed tomography image (right) confirms traumatic aortic injury (arrow) with associated mediastinal haematoma (arrowhead) and a large left haemothorax (H).
Many requested investigations do not alter the patient’s management, and in some cases they may be misleading. In head injuries, there is virtually no indication for performing a skull radiograph. Most patients who have sustained a substantial head injury should have a computed tomography scan. A safe approach to head injuries is always to scan it.
Command 3 Skull radiographs are not usually needed when dealing with head injuries. Important findings are generally subtle and often missed. This patient has a depressed skull fracture (arrow).

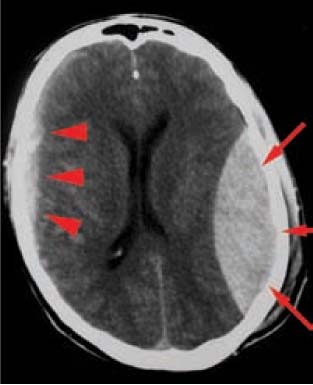
Command 3 Computed tomography image of head shows large left extradural haematoma (arrow) and subtle large right subdural haematoma (arrowhead).
Look at the radiograph properly, not be biased, and use a systematic approach. Always get the clinical history before giving an opinion. Then you will often pick up abnormalities that you may otherwise have missed. Never rely on someone else’s opinion or report on radiographs if you have not seen the radiographs yourself. This is particularly relevant when patients are handed over at the end of a shift or when patients are transferred from elsewhere.
In a pressured environment such as an emergency department, it is easy to rush and make mistakes. Interpreting radiographs too quickly inside a badly lit, noisy room with many distractions is a recipe for disaster. Interpretation of radiographs should be done in a calm manner in a quiet, well lit room using a viewing box or monitor. A common problem is that the person assessing the radiograph will focus immediately on expected abnormalities.
Even knowing the clinical history, try to ignore it at first and use a systematic approach. It is critical though that you always get the clinical history before giving your final opinion or report, because you must try to interpret the radiological findings in the context of the clinical presentation and answer the question.
Review the radiographic findings in conjunction with the patient’s history and your clinical findings. If the radiograph does not fit, review the history and clinical findings or ask for help. Many cases require further imaging – for example, request a magnetic resonance scan or an isotope bone scan in an elderly patient with a suspected fracture of the neck of femur, even if the initial plain radiographs seem normal.
Command 6 Anteroposterior view of right hip showing subtle fracture of neck of femur (arrow), which was missed initially (left) and later confirmed on isotope bone scan as a fracture (arrowhead).
