Contents
Foreword
Preface
Dedications
Part 1
Case histories
ECG interpretations and comments
Part 2
Case histories
ECG interpretations and comments
Appendix A: Differential diagnoses
Appendix B: Commonly used abbreviations
Index

© BMJ Publishing Group 2003
BMJ Books is an imprint of the BMJ Publishing Group
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording and/or otherwise, without the prior written permission of the publishers.
First published in 2003
by BMJ Books, BMA House, Tavistock Square,
London WC1H 9JR
www.bmjbooks.com
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British Library
ISBN 0 7279 1654 8
Foreword
There has been a great need for a user friendly ECG text that fills the void between an introductory text designed for students and an advanced reference source for cardiologists. “ECGs for the Emergency Physician” fills this void. It is an ECG teaching and reference textbook for acute and emergency care physicians written by two specialists practicing and teaching acute and emergency care.
Drs Mattu and Brady have created an ECG text that facilitates self instruction in learning the basics, as well as the complexities, of ECG interpretation. They know that ECG interpretation requires knowledge, insight and practice. They know “the eye does not see, what the mind does not know.” In order to accomplish this goal of teaching ECG interpretation, they have divided their book into two parts. In Part I, as the authors state, are the “bread and butter” ECGs of acute care. These are the ECG findings that form the core knowledge necessary for accurate ECG interpretation. In Part II they teach recognition of more subtle ECG abnormalities, which when mastered, allow the practitioner to become an expert.
The beauty of this text lies in the combining of a collection of emergency department ECGs with the authors’ insights and expert observations. This book has great utility as a reference text, a bound ECG teaching file, a board review aide or a resident in emergency medicine’s best friend for learning the art of advanced ECG interpretation. Its greatest value however, is for all of us who want to be both challenged and taught by 200 great electrocardiograms and their interpretations.
May the forces be with you.
Corey M Slovis
Professor of Emergency Medicine and Medicine
Chairman, Department of Emergency Medicine
Vanderbilt Medical Center
Nashville, Tennessee
Medical Director Metro Nashville Fire EMS
Preface
Emergency and other acute care physicians must be experts in the use and interpretation of the 12-lead electrocardiogram (ECG). We have prepared this text with this basic though highly important thought in mind. This text represents our effort to further the art and science of electrocardiography as practiced by emergency physicians and other acute care clinicians.
A significant number of the patients managed in the emergency department and other acute care settings present with chest pain, cardiovascular instability, or complaints related to the cardiovascular system. The known benefits of early, accurate diagnosis and rapid, appropriate treatment of cardiovascular emergencies have only reinforced the importance of physician competence in electrocardiographic interpretation. The physician is charged with the responsibility of rapid, accurate diagnosis followed by appropriate therapy delivered expeditiously. This evaluation not infrequently involves the performance of the 12-lead ECG. For example, the patient with chest pain presenting with ST-segment elevation, acute myocardial infarction must be rapidly and accurately evaluated so that appropriate therapy is offered in prompt fashion. Alternatively, the hemodynamically unstable patient with atrioventricular block similarly must be cared for in a rapid manner. In these instances as well as numerous other scenarios, resuscitative and other therapies are largely guided by information obtained from the ECG.
The electrocardiogram is used frequently in the emergency department (ED) and other acute care settings; numerous presentations may require a 12-lead electrocardiogram. For instance, the most frequent indication for ECG performance in the ED is the presence of chest pain; other complaints include dyspnea and syncope. Additional reasons for obtaining an ECG in the ED include both diagnosis-based (acute coronary syndrome, suspected pulmonary embolism, and the “dysrhythmic” patient) and system-related indications (for the “rule-out myocardial infarction” protocol, for admission purposes, and for operative clearance).1 Regardless of the cause, the physician must be an expert in the interpretation of the 12-lead ECG. Interpretation of the ECG is as much an art as it is a science. Accurate ECG interpretation requires a sound knowledge of the electrocardiogram, both the objective criteria necessary for various diagnoses of those patients encountered in the ED as well as a thorough grasp of the various electrocardiographic waveforms and their meaning in the individual patient.
We have prepared this text for the physician who manages patients not only in the ED but also in other acute care settings – whether it be in the office, the hospital ward, critical care unit, the out-of-hospital arena, or other patient-care locale. We have used actual ECGs from patients treated in our EDs; a brief but accurate history has also been provided in each instance. In certain cases, the history may provide a clue to the diagnosis yet in other situations the clinical information will have no relationship to the final diagnosis – as is the case in the ED. We have made an effort to choose the most appropriate ECG from each patient, but as occurs in “real ED,” some of the ECGs are imperfect: the evaluation is hindered by artifact, incomplete electrocardiographic sampling, etc. We have also provided the ECGs in a random fashion, much the way actual patients present to the emergency department. We have endeavored to reproduce the reality of the ED when the reader uses this text to expand their knowledge of the 12-lead electrocardiogram and how it relates to patient care.
The reader is advised to read the clinical history provided for each ECG and then, much as the clinician would interpret the electrocardiogram in the ED, review the 12-lead ECG. After a clinically focused review of the ECG, the reader is then able to review the interpretation. This ECG text has been constructed in two basic sections. The first half of the text contains ECGs that we feel represent the “bread and butter” of emergency electrocardiography – the core material with which we feel that the acute care physician must be thoroughly familiar. These ECGs were chosen because they represent common electrocardiographic diagnoses that all emergency physicians should know. This section is prepared primarily for the physician-in-training (for example, the emergency medicine resident) though practicing physicians will also benefit from reviewing the material. The second half of the text is composed of ECGs that are more challenging. The electrocardiographic diagnoses are more difficult to establish and will often be on subtle findings. In some cases, the ECGs in this section were chosen not necessarily because of the related level of difficulty but because of subtle teaching points found, which are likely to be beyond the level of the physician-in-training.
It is also crucial to understand that this text is not intended for the “beginner in ECG interpretation”. The text, in essence an electrocardiographic teaching file, is intended for the physician who possesses a sound, basic understanding of electrocardiography yet desires additional practice and review – a review which is highly clinically pertinent. The electrocardiography beginner is advised to begin by reading through one of the many outstanding books that have previously been written for novice students prior to studying this teaching file.
One last point must also be stressed to the reader of this text. Diagnostic criteria for various electrocardiographic diagnoses vary somewhat amongst authors. Therefore, in an effort to standardize the interpretations used in this text, we chose to use the following two references as the “gold standard” for electrocardiographic interpretations: Chou and Knilans’ Electrocardiography in Clinical Practice: Adult and Pediatric and Galen’s Marriott’s Practical Electrocardiography.2,3
References
1. Brady W, Adams M, Perron A, Martin M. The impact of the 12-lead electrocardiogram in the evaluation of the emergency department patient. Ann Emerg Med (accepted for publication/publication pending).
2. Chou T-C, Knilans TK. Electrocardiography in Clinical Practice: Adult and Pediatric 4th edn. Philadelphia, PA:WB Saunders Company, 1996.
3. Galen SW. Marriott’s Practical Electrocardiography 10th edn. Philadelphia, PA: Lippincott Williams & Wilkins, 2001.
Dedications
This work is dedicated to my wife, Sejal, for her tremendous patience and never-ending support; to my son, Nikhil, for constantly reminding me of the priorities in life; to the Emergency Department staff at Mercy Medical Center in Baltimore for their friendship and their ECG contributions; to the faculty and residents of the University of Maryland Emergency Medicine Residency Program for providing the main inspiration for this work; to Mary Banks and BMJ Books for supporting and believing in this work; to Dr Bill Brady for his mentorship, friendship, and commitment to teaching and education; and to emergency physicians around the world – may your dedication to learning continue to strengthen our specialty and improve patient care.
Amal Mattu
Director, Emergency Medicine Residency Program
Co-Director, Emergency Medicine/Internal Medicine Combined Residency Program
University of Maryland School of Medicine
Baltimore, Maryland
USA
I would like to thank my wife, King, for her love, support, wise counsel, and patience – none of this effort would be possible without her; my children, Lauren, Anne, Chip, and Katherine, for being wonderful and my primary inspiration; my parents, Bill and Joann Brady, for all that they have done and continue to do; the Emergency Medicine Residents (past, present, and future) at the University of Virginia, for their hard work, astronomical dedication, and inspiration – all directed at our patients and the specialty of Emergency Medicine; Dr Marcus Martin, Chair of Emergency Medicine at the University of Virginia, for his support, guidance, and mentorship; and my co-author, Dr Amal Mattu, for his dedicated effort on this book in particular and his dedication to Emergency Medicine education in general – a true gentleman, talented clinician, and distinguished scholar
William Brady
Associate Professor, Vice Chair, and Program Director
Department of Emergency Medicine
University of Virginia Health System
Charlottesville, Virginia
USA
and
Medical Director, Charlottesville-Albermarle
Rescue Squad, Charlottesville, Virginia,
USA
Part 1
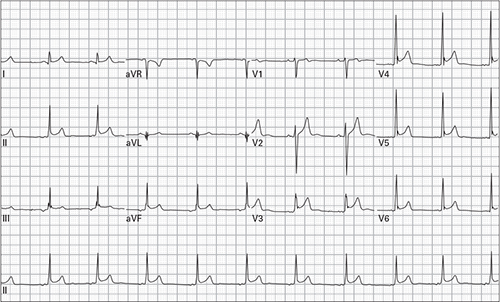
1. 45 year old woman, asymptomatic

2. 24 year man with chest ache after lifting weights

3. 76 year old man with dyspnea

4. 64 year old man, asymptomatic

5. 48 year old woman reports severe lightheadedness with walking; she recently started a new medication for hypertension

6. 79 year old man 45 minutes after receiving thrombolytic therapy for acute myocardial infarction; currently pain-free

7. 43 year old man, asymptomatic

8. 82 year old man recently increased his dose of a beta-receptor blocking medication; he now reports exertional lightheadedness

9. 49 year old man with occasional episodes of chest pain

10. 65 year old woman with a long history of smoking presents for treatment of an emphysema exacerbation

11. 54 year old woman complains of midsternal chest pain and lightheadedness

12. 86 year old woman complains of generalized weakness

13. 61 year old man with palpitations and lightheadedness

14. 44 year old woman with intermittent episodes of palpitations

15. 24 year old pregnant woman with three days of frequent vomiting

16. 37 year old man with pleuritic chest pain

17. 63 year old man with palpitations and lightheadedness

18. 33 year old obese man with sharp chest pain and dyspnea

19. 81 year old woman with palpitations and generalized weakness

20. 61 year old man, asymptomatic
21. 57 year old woman with mild chest pain and palpitations

22. 75 year old man presents with cough, dyspnea, and wheezing

23. 43 year old man with severe palpitations

24. 52 year old homeless, alcoholic man found lying in an alley

25. 68 year old man with history of congestive heart failure complains of dyspnea

26. 85 year old woman reports a recent syncopal episode

27. 40 year old woman with palpitations and lightheadedness

28. 35 year old woman with dyspnea

29. 41 year old woman with chest pain after cocaine use

30. 57 year old man with chest pressure and diaphoresis

31. 57 year old man with chest pressure and diaphoresis (right-sided precordial leads)

32. 60 year old woman with acute onset of expressive aphasia

33. 54 year old man 24 hours after receiving thrombolytic therapy for acute myocardial infarction; currently asymptomatic

34. 41 year old woman with nausea and vomiting

35. 75 year old woman accidentally took too many of her beta-blocker tablets

36. 68 year old man with palpitations and generalized weakness

37. 38 year old man with chest pain, nausea, and diaphoresis

38. 62 year old woman with palpitations

39. 74 year old man with chest pain and palpitations

40. 45 year old man with severe left chest pressure, nausea, and dyspnea

41. 45 year old man with left chest pressure

42. 85 year old woman presents after a syncopal episode, still reports lightheadedness

43. 81 year old man being admitted for pneumonia

44. 71 year old woman with chronic renal insufficiency presents with carpopedal spasm

45. 46 year old man with chest and left arm pain, vomiting, and diaphoresis

46. 53 year old diabetic woman with four days of nausea, vomiting, and lightheadedness

47. 85 year old woman with chest pain

48. 66 year old man with severe lightheadedness and diaphoresis

49. 58 year old man with congestive heart failure reports increasing dyspnea and lower extremity edema

50. 43 year old man reports eight hours of left chest and arm pain

51. 52 year old woman with chest pain

52. 62 year old man with renal failure complains of progressive dyspnea and orthopnea after missing his last two hemodialysis sessions

53. 47 year old man with palpitations and dyspnea

54. 48 year old woman presents after a clonidine overdose

55. 23 year old man reports dyspnea and palpitations

56. 57 year old man reports generalized weakness and palpitations

57. 54 year old man with five days of anorexia, nausea, and vomiting

58. 66 year old woman with epigastric pain, nausea, dyspnea, and diaphoresis

59. 70 year old woman with nine hours of chest pain and dyspnea

60. 52 year old alcoholic woman presents with frequent vomiting

61. 45 year old woman with palpitations and lightheadedness

62. 45 year old man with severe lightheadedness

63. 52 year old man with sharp chest pain

64. 71 year old woman with generalized weakness

65. 34 year old woman presents unconscious with respiratory depression and pinpoint pupils

66. 36 year old woman has had intermittent episodes of palpitations and lightheadedness

67. 70 year old woman with chest discomfort and generalized weakness

68. 41 year old man with end-stage renal failure presents with generalized weakness after missing his last three hemodialysis sessions

69. 45 year old woman with left chest and arm pain and dyspnea

70. 78 year old woman with dyspnea and nausea

71. 75 year old woman presents after a syncopal episode

72. 50 year old woman with chest pain and diaphoresis for five hours

73. 59 year old man presents with dyspnea, cough, and hypoxia

74. 62 year old woman with chest pain and severe dyspnea gradually worsening for three days

75. 40 year old man with sharp left-sided chest pain and dyspnea

76. 28 year old woman with palpitations and chest pain

77. 53 year old man with left arm “squeezing sensation” and nausea for eight hours

78. 69 year old woman with severe nausea and dyspnea

79. 68 year old man presents unconscious with blood pressure 108/60

80. 65 year old woman with “funny feeling in chest”

81. 55 year old woman with occasional syncopal episodes and a recent episode of palpitations

82. 69 year old man with dyspnea and diaphoresis

83. 79 year old man with abdominal pain

84. 85 year old man with palpitations and fatigue

85. 63 year old man with epigastric burning, belching, diaphoresis, and lightheadedness

86. 70 year old man with dyspnea and generalized weakness

87. 70 year old woman with nausea, vomiting, and diaphoresis

88. 55 year old morbidly obese woman with generalized abdominal pain

89. 44 year old chronic alcoholic with persistent vomiting; becomes unresponsive during the ECG

90. 25 year old woman with palpitations and lightheadedness
91. 28 year old woman eight weeks pregnant presents with chest pain, dyspnea, and blood pressure 80/40

92. 47 year old woman with chest pain; now pain free after use of sublingual nitroglycerin

93. 38 year old woman with chest pain, dyspnea, fever, and productive cough

94. 46 year old woman with episodic palpitations, frequent diaphoresis, and a 15 pound weight loss over the past one month

95. 84 year old woman with nausea and vomiting

96. 57 year old man with chest pressure, dyspnea, and nausea

97. 57 year old man with chest pressure, dyspnea, and nausea (right-sided precordial leads)

98. 45 year old woman with eight hours of chest and left neck pain

99. 24 year old woman had a syncopal episode after seeing blood; she has no pain
100. 26 year old woman with history of renal failure reports generalized weakness and nausea

(Rates refer to ventricular rates unless otherwise specified; axis refers to QRS axis unless otherwise specified)