Contributors
Preface to Fifth Edition
1 Pain in the Ear
Acute otitis externa
Acute suppurative otitis media
Acute (coalescent) mastoiditis
Other complications of acute suppurative otitis media
Chronic secretory otitis media (otitis media with effusion)
‘Malignant’ otitis externa
Other causes of pain
Further reading
2 Discharge from the Ear
Acute otitis media
‘Subacute’ suppurative otitis media
Chronic otitis externa
Chronic suppurative otitis media
Recognition and treatment of safe ears
Treatment of unsafe ears
Discharge from a mastoid cavity
Further reading
3 Hearing Impairment and Tinnitus in Adults
Conductive deafness
Sensorineural deafness
Assessment
Management
Tinnitus
Further reading
Further resources
4 Adult Hearing Rehabilitation and Cochlear Implants
Hearing tactics
Hearing aids
Environmental aids
Cochlear implants
Further reading
Further resources
5 Childhood Hearing Loss
Introduction
Early detection of hearing loss: universal neonatal screening
Early provision of hearing aids
Further investigations in neonatal deafness
Childhood audiometry
Otitis media with effusion/middle ear effusion – ‘glue ear’
Tympanostomy tubes (grommets)
Adenoidectomy
Other causes of conductive deafness in children
Bone-anchored hearing aids for conductive hearing loss
Cochlear implants for profound hearing loss
Education and support
Further reading
6 Acoustic Neuromas and other Cerebello Pontine Angle Tumours
The cerebello pontine angle
The natural history of acoustic neuromas
The symptoms and signs of acoustic neuromas
Diagnosis
Management
Further reading
7 Vertigo
Menière’s disease
Benign paroxysmal positional vertigo
Sudden vestibular failure
Migraine
Assessment
Symptomatic treatment of vertigo
Further reading
8 Facial Palsy
Anatomy
Presentation
Aetiology
Bell’s palsy
Prognosis
Herpes zoster oticus (Ramsay Hunt syndrome)
Otitis media
Lyme disease
Neoplasms
Trauma
Other causes
Further reading
9 Paranasal Sinus Diseases and Infections
Sinus anatomy and mucociliary pathways
Clinical definition of rhinosinusitis
Aetiology
Nasal polyposis
Clinical presentation of paranasal sinus disease
Differential diagnosis
Investigations
Imaging
Complications of rhinosinusitis
Treatment
Further reading
Further resources
10 Facial Pain
Tension-type headache
Midfacial segment pain
Pain arising from the sinuses
Proposed theories for the aetiology of rhinological pain
Pain following trauma or surgery
Migraine
Cluster headache
Chronic paroxysmal hemicrania
Eye-related pain
Teeth, jaws and related structures
Trigeminal neuralgia
Atypical facial pain
Headache and sinusitis
Conclusions
Further reading
11 Sore Throats
Throat symptoms
Presentation
Diagnosis and treatment
Indications for tonsillectomy
Sore throats with cervical adenopathy
Complications of throat sepsis
Sore throat with acute airway distress
Sore throat with subacute airway obstruction
Sore throat with a chronic upper airway obstruction
Pharyngitis
Oral mucosal lesions
Further reading
12 Breathing Disorders
Pathophysiology
Stridor in children
Evaluation of stridor in adults
Surgical management of the acutely obstructed airway
Further reading
13 Swallowing Problems
Swallowing and its mechanisms
Symptoms
Clinical evaluation
Presbyphagia
Globus pharyngeus
Pharyngeal pouch (Zenker’s diverticulum)
Postcricoid web
Neurological diseases
Percutaneous gastrostomy
Swallowing therapy
Further reading
14 Snoring and Obstructive Sleep Apnoea
Spectrum of the condition
Aetiology
Consequences of sleep-related breathing disorders
Assessment
Treatment options
Snoring and obstructive sleep apnoea in children
Key points
Further reading
15 Hoarseness and Voice Problems
Anatomy, physiology and pathophysiology
Aetiology of voice problems
Guidelines and referral
Assessment
Treatment
Structural/neoplastic conditions
Inflammatory conditions
Neuromuscular conditions
Muscle tension imbalance conditions
Conclusions
Further reading
16 Trauma, Injuries and Foreign Bodies
Ear
Nose
Neck
Throat/oro-hypopharynx
Tracheo-bronchus
Oesophagus
Further reading
17 Epistaxis, Catarrh, Glossodynia, Halitosis and Somatization
Epistaxis
Catarrh and postnasal drip
Burning mouth syndrome and glossodynia
Halitosis
Somatization
Further reading
18 Neck Swellings
Surgical anatomy of the neck
Diagnosis
Examination
Diagnostic studies
Characteristics of non-malignant neck lumps
Indications for specialist referrals
Further reading
19 Head and Neck Cancer
Definition
Incidence
Symptoms and signs
Uncommon head and neck cancers
Risk factors
Prognostic factors
Staging and evaluation
Management of oral cavity cancer
Management of laryngeal cancer
Management of hypopharyngeal cancer
Quality of life
Prognosis
Further reading
Further resources
Index
© 2007 by Blackwell Publishing Ltd
BMJ Books is an imprint of the BMJ Publishing Group Limited, used under licence
Blackwell Publishing, Inc., 350 Main Street, Malden, Massachusetts 02148-5020, USA
Blackwell Publishing Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UK
Blackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton, Victoria 3053, Australia
The right of the Author to be identified as the Author of this Work has been asserted in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
First published 1981
Second edition 1988
Third edition 1993
Fourth edition 1997
Fifth edition 2007
1 2007
Library of Congress Cataloging-in-Publication Data
ABC of ear, nose, and throat / edited by Harold Ludman and Patrick J. Bradley. 5th ed. p. ; cm.
Rev. ed. of: ABC of otolaryngology / Harold Ludman. 1997. Includes bibliographical references and index. ISBN 978-1-4051-3656-3
1. Otolaryngology. I. Ludman, Harold. II. Bradley, Patrick J., 1949-III. Ludman, Harold. ABC of otolaryngology. [DNLM: 1. Otorhinolaryngologic Diseases. WV 140 A134 2007]
RF46.A2344 2007 617.5'1--dc22
2006036143
ISBN: 978-1-4051-3656-3
A catalogue record for this title is available from the British Library
Cover image is courtesy of and adapted from University of Nebraska Medical Centre
Associate Editor: Vicki Donald
Editorial Assistant: Victoria Pittman
Production Controller: Rachel Edwards
For further information on Blackwell Publishing, visit our website: www.blackwellpublishing.com
Blackwell Publishing makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check that any product mentioned in this publication is used in accordance with the prescribing information prepared by the manufacturers. The author and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this book.
Contributors
David Albert
Consultant Paediatric ENT Surgeon, Great Ormond Street Hospital, London, UK
Declan Costello
Specialist Registrar, John Radcliffe Hospital, Oxford, UK.
Kevin Gibbin
Consultant ENT Surgeon, Queens Medical Centre, Nottingham, UK
Nick S Jones
Consultant Rhinologist, Queens Medical Centre, Nottingham, UK
Julian McGlashan
Consultant ENT Surgeon, Queens Medical Centre, Nottingham, UK
William McKerrow
Consultant ENT Surgeon, Raigmore Hospital, Inverness, UK
Antony Narula
Consultant ENT Surgeon and Head of Department, St Mary's Hospital, London; Honorary Professor of Otolaryngology, Middlesex University, UK
Vinidh Paleri
Consultant Surgeon, Otolaryngology-Head and Neck Surgery, Newcastle upon Tyne University Hospitals, Newcastle, UK
Parag M Patel
Specialist Registrar, Royal Surrey County Hospital, Guildford, Surrey, UK
Shahed Quraishi
Consultant Head and Neck Surgeon, Doncaster Royal Infi rmary, Doncaster, UK
Julian Rowe-Jones
Consultant Rhinologist and Nasal Plastic Surgeon, Guildford Nuffield Hospital, Guildford, Surrey, UK
Anshul Sama
Consultant Rhinolaryngologist, Queens Medical Centre, Nottingham, UK
Iain Swan
Consultant ENT Surgeon, Gartnavel General Hospital, Glasgow, UK
Archana Vats
Specialist Registrar, St Mary's Hospital, London, UK
Anthony Wright
Professor of Otolaryngology, Institute of Laryngology and Otology, University College London, London, UK
Preface to Fifth Edition
The first edition of this small volume, The ABC of Ear, Nose and Throat, was derived 25 years ago from a series of articles published at that time in the British Medical Journal to present the substance of this important speciality in an easily assimilable form for a wide readership of general practitioners, medical students, nurses and all those many sprouting paramedical specialties involved with speech, hearing, and head and neck disorders. This target readership has not changed, but the specialty, like most others, has expanded and developed subspecialties in all its divisions.
Otology has changed from the exciting renaissance of microscopic middle ear work that began in the 1960s at the start of my personal otological career, to the amazing developments that include cochlear implantation for inner ear deafness, and neuro-otology has extended from the management of peripheral labyrinthine disorders to embrace surgery within the base of the skull.
Rhinological change has brought us the endoscopic techniques that have revolutionized treatment for paranasal sinus diseases, while the management of throat malignancy has evolved out of all recognition into today’s comprehensive management of head and neck tumours.
It is entirely appropriate therefore that, for this expanded fifth edition, Patrick Bradley FRCSIr, FRCSEd, FRCSEng, MBA, as an internationally recognized authority on head and neck diseases and their treatment, should have become the joint editor, and that several specialists, recognized as experts in various subspecialties, have been enlisted to write about them.
The title has appositely reverted to its briefer, earlier one of ENT, which is so quintessentially British and which trips much more readily off the tongue than does otolaryngology.
Harold Ludman
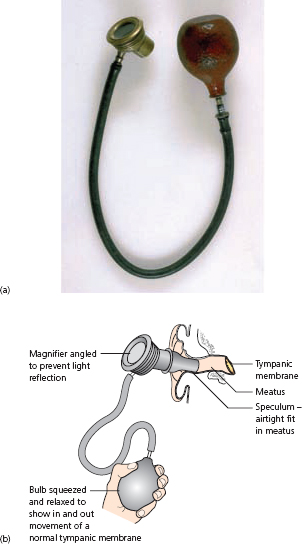
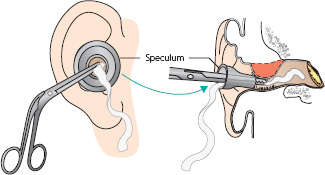
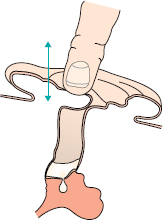
Pain is one of six symptoms that may indicate ear disease (Box 1.1). Inflammatory causes of pain are recognized by inspection of the external ear and tympanic membrane. An otoscope is usually used in general practice, but otologists always use a headlight or head mirror to provide vision coincident with the direction of illumination, allowing manipulation with freed hands and instruments for the removal of wax or debris, and for the assessment of drum mobility with a pneumatic speculum (Fig. 1.1).
A binocular microscope is invariably used for fine manipulation with micro instruments and suction apparatus for accurate assessment under magnification of six times or more (Fig. 1.2).
If the external ear canal and the tympanic membrane are definitely normal, then pain cannot arise from ear disease. The reliability of this judgement depends on the skill and experience of the examiner. A tympanic membrane may show subtle changes, which are not easily recognized, while some abnormalities are irrelevant. If in any doubt, an otological opinion should be sought (Fig. 1.3).
Figure 1.1 (a) Photograph of pneumatic (Siegle’s) speculum and (b) diagram showing its use.
Acute otitis externa may be either diffuse – involving all the skin of the external meatus – or localized as a furuncle (Fig. 1.4).
Figure 1.2 Binocular microscope with sidearm for observer.
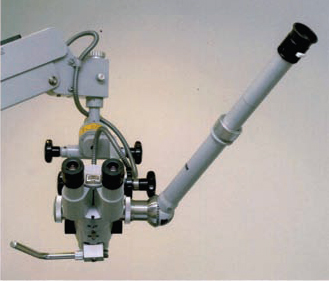
Figure 1.3 (a) Photograph of normal left tympanic membrane and (b) labelled diagram.
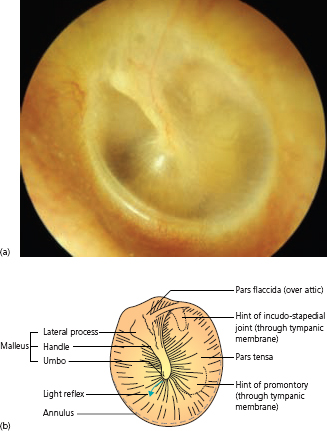
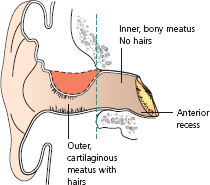
A furuncle is a very tender swelling (a boil). It is always in the outer ear canal, as there are no hair follicles in the inner bony meatus. Hearing is impaired only if the meatus becomes blocked by swelling or discharge, and fever occurs only if infection spreads in front of the ear, as cellulitis or erysipelas. Superficially tender enlarged nodes may be palpable in front of or behind the ear. The pinna is tender to movement in acute otitis externa, but this is not the case in acute otitis media. Discharge, if any, is usually thick and scanty, unlike the copious mucoid discharge through tympanic membrane perforation from acute middle ear infections. Fungal skin infections cause severe pain with wet keratin desquamation and black or coloured granules of the fruiting heads of conidiophores.
Figure 1.4 Furuncle in external auditory meatus.
Systemic antibiotics are advised in acute otitis externa only if there is fever or lymphadenitis. Sometimes, meatal swelling must be reduced by inserting a ribbon gauze wick painted with a deliquescent substance such as magnesium sulphate paste, or glycerine and 10% ichthammol (Fig. 1.5). Proprietary ‘Pope’ wicks (Xomed) are thin and stiff to enable careful insertion, and they then soften and swell gently when moistened with liquid medication. A wick should be replaced daily until skin swelling subsides. Ear drops may then be used – either aluminium acetate to ‘toughen’ the skin or topical antibiotics, such as gentamicin, framycetin or neomycin, combined with steroids. Topical clotrimazole is a useful antifungal agent. Systemic analgesics, together with warmth, applied through a hot pad or heat lamp, relieve pain. Recurrent furunculosis should raise a suspicion of diabetes.
Figure 1.5 Inserting a wick.
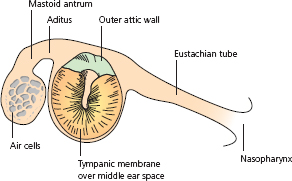
Acute suppurative otitis media causes deep-seated pain, impaired hearing and systemic illness with fever. A blocked feeling in the ear then pain and fever, are followed by discharge if the tympanic membrane perforates – with relief of pain. The whole middle ear cleft is affected. This is the entire air-containing space comprising the Eustachian tube, the middle ear cavity, the mastoid antrum and its adjacent mastoid air cells (Fig. 1.6). For this reason, deep pressure over the mastoid antrum elicits tenderness in acute otitis media; this does not imply the development of mastoiditis. Bacterial infection is usually by Streptococcus pneumoniae, or Haemophilus influenzae in very young children. Diagnosis is made by inspecting the tympanic membrane, but this may be prevented by wax, or by swelling from a secondary otitis externa. Only if the whole drum can be certified as normal and there is no conductive hearing loss (demonstrated by tuning fork tests) can otitis media confidently be excluded. Adjacent lymph nodes are never enlarged in simple otitis media.
Systemic antibiotics are recommended. The commonest infecting organisms are Streptococcus pneumoniae, Haemophilus influenzae and Moraxella (Branhamella) catarrhalis. The antibiotic of choice, effective against all these, is amoxycillin. If β lactamase-producing organisms are likely, amoxycillin combined with clavulanic acid (Augmentin) or trimethoprin and sulphamethoxazole may be preferred. Oral administration is advised, even for the first dose, and medication must be continued for at least 5 days. Supplementary treatment includes pain relief by analgesics and warmth. Warm olive oil drops are soothing. If the tympanic membrane perforates, the ensuing discharge should be cultured, but an antibiotic should be changed on clinical and not bacteriological grounds. Rarely, the drum may bulge under pressure without rupture, requiring urgent incision to release pus (myringotomy).
Recurrent acute otitis media may be provoked by predisposing causes, such as persisting middle ear effusions, when a potentially infected accumulation of mucus persists in the middle ear cleft. Myringotomy with insertion of a ventilation tube or ‘grommet’ may then be advisable. Adenoid enlargement with repeated infection is probably also a causative factor, but the role of adenoidectomy remains controversial. In the absence of predisposing factors, each attack should be treated as it arises. After any episode, return to normal is expected and should be confirmed within 3 weeks.
Figure 1.6 The middle ear cleft.
Acute mastoiditis is caused by the breakdown of the thin bony partitions (trabeculae) between the mastoid air cells, which then become coalescent (Fig. 1.7). This process takes 2–3 weeks to occur fully. Throughout that time, there is, in most cases, continuing and increasingly copious discharge through a perforation in the drum, with general malaise and fever, unless this has been suppressed by antibiotics. If a patient has pain a few days after the tympanic membrane has been reliably judged to be normal, then that patient cannot have developed mastoiditis. Difficulties arise when a patient is thought to have recovered from acute otitis media, but in reality the condition has ‘grumbled on’, perhaps by suppression of systemic effects with antibiotics. Mastoiditis should be suspected in any patient with continuous discharge from the middle ear for over 10 days, particularly if he or she is continually unwell.
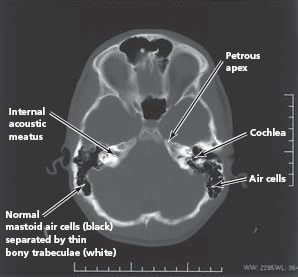
Radiographs or, better, CT scans of the mastoid air cells may help to diagnose the condition, but not always. Only if they show a clearly aerated normal cell system (Fig. 1.8) can mastoiditis be excluded. The classical appearance of breakdown of intracellular trabeculae is not always apparent. Otitis externa may cause apparent haziness of the air cell system because of oedema of the soft tissues over the mastoid process. The often-described traditional classical sign of a swelling behind the ear with downward displacement of the pinna implies a subperiosteal abscess. This is a complication rather than a feature of mastoiditis. A subperiosteal abscess can also, by erosion of the bony outer attic wall, cause swelling in the roof of the deep part of the external ear canal, in contrast with a furuncle, which arises only in its outer part. If any doubt persists after mastoid imaging, surgical exploration is advisable.
Figure 1.7 Breakdown of mastoid air cells.
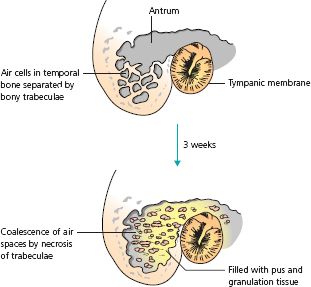
Figure 1.8 CT scan of normal mastoid air cells.
These are all also possible complications of the bone erosive forms of chronic suppurative otitis media (see Chapter 2 and Fig. 1.9). They arise if infection spreads beyond the middle ear cleft itself. Complications occurring within the petrous temporal bone include facial palsy, suppurative labyrinthitis and lateral sinus thrombophlebitis; those occurring within the cranial cavity are meningitis, extradural abscess, subdural abscess and brain abscess (in the temporal lobe or cerebellum).
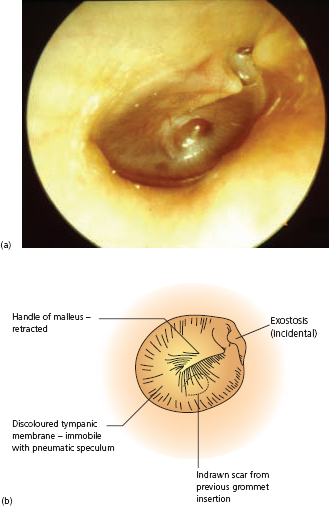
Niggly, short-lived pain is a common feature of ‘glue ear’. The drum looks abnormal because of the effusion (Fig. 1.10). Classically, there is injection with visible radial vessels, which may prompt a misdiagnosis of otitis media. The colour may be yellowish or sometimes blue. The child is well and afebrile, however, and the associated hearing loss has usually been recognized for some time.
Figure 1.9 Complications of suppurative otitis media.
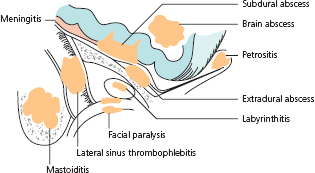
Figure 1.10 (a) Photograph of tympanic membrane with ‘glue ear’ and (b) labelled diagram.
An essential diagnostic feature, which can be elicited by an otologist using a headlight and a pneumatic speculum, is altered mobility of the tympanic membrane. It may be totally immobile when external ear canal air pressure is raised and reduced, or there may be sluggish outward movement followed by a rapid ‘snap’ back when the partial vacuum is released. This altered mobility can also be demonstrated by tympanometry using an impedance measuring meter during continuously changing ear canal pressure – from above to below normal atmospheric level. Simple, automatic tympanometers print out a quickly available chart indicating middle ear air pressure and its changes (if any) as the external ear air pressure is raised and then lowered. However, there can be technical problems in using these devices reliably.
This is a rare but serious form of infection (not neoplastic, despite the name), caused by Pseudomonas aeruginosa, arising usually in elderly diabetics. It should be suspected if patients in this group suffer severe pain, excessive for the signs of otitis externa. Infection invades the bony base of the skull and adjacent soft tissues. Facial paralysis and other cranial nerve palsies may develop, and mortality used to be high. A suspicious finding is granulation tissue in the ear canal, which must be investigated by CT scanning. Treatment with intravenous gentamicin, or with oral ciprofloxacin, is administered continuously for several weeks, and must not cease before recovery from pain.
Bullous myringitis is another cause of severe pain. Viral (probably influenzal) infection causes haemorrhagic blistering of the ear drum and external ear canal. There is often an associated haemorrhagic effusion in the middle ear and it may be difficult to distinguish this condition from otitis media. For that reason alone antibiotics may be administered, but the only necessary treatment is potent analgesia.
If the external ear canal and drum are normal, with normal movement of the drum on examination with a pneumatic speculum, pain cannot be due to disease of the ear. It may well be referred from territory sharing its ultimate sensory innervation with the outer or middle ear (Fig. 1.11). Pain therefore may arise from:
Figure 1.11 Origins of referred pain.
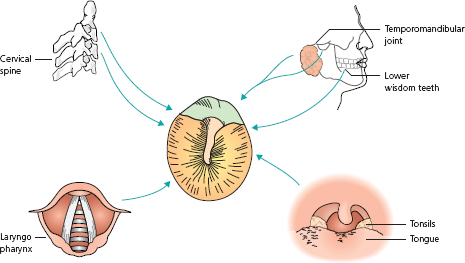
If there is no inflammatory ear disease and no disease in sites from which pain might be referred to the ear, remaining possibilities include glossopharyngeal neuralgia, migrainous neuralgia or psychogenic pain.
Often no cause can be found; it may sometimes be attributed to depression and a trial of antidepressive medication can be advised.
Kerr A, Booth J. (eds) (1997) Scott Brown’s Otolaryngology, 6th Edition. Butterworth-Heinemann, Oxford.
Ludman H, Wright T. (eds) (1998) Diseases of the Ear, 6th Edition. Arnold-Hodder Headline, London.
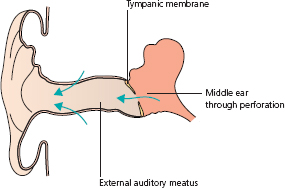
Discharge from the ear (otorrhoea) can suggest acute otitis externa or otitis media, and is usually the main feature of chronic inflammatory diseases of the external ear or middle ear (Box 2.1 and Fig. 2.1).
In acute disease, pain invariably dominates and precedes discharge (see Chapter 1).
Acute suppurative otitis media produces profuse mucopurulent or purulent discharge after the pain, if the drum perforates. As the perforation heals, the discharge ceases.
Figure 2.1 Where does discharge come from?
Increasingly profuse discharge persisting for more than 10 days may suggest acute coalescent mastoiditis, especially if the patient is febrile with deep tenderness over the mastoid antrum, behind the pinna (see Chapter 1).
Now that acute mastoiditis is rare, a common syndrome is that of a ‘well’ child continuously discharging mucopus from the ear for three or more weeks after a typical attack of acute suppurative otitis media. Often, grommets have been sited in the ear drum. Continuing mucosal infection of the middle ear by resistant organisms, continuing infection of the nasopharynx with secondary infection of the middle ear cleft, and changes in the mucosa of the middle ear secondary to Eustachian tube dysfunction may all contribute. A grommet may be irritating the adjacent tissues, suggested by adjacent granulation tissue visible to inspection, around its edges on the surface of the tympanic membrane.
Swab culture will indicate appropriate antibiotics to give systemically. After regular gentle toilet to remove infected debris from the meatus, topical antibiotic and steroid drops should be massaged into the middle ear by pressure on the tragus, for 5–7 days (Fig. 2.2).
Children should learn to blow their noses to prevent mucus stagnation with infection. Decongestant nasal sprays may help, after blowing the nose, for a short period only – up to a week. Systemic antihistamines may also be part of the regimen, to reduce allergic swelling of the mucosa around the orifice of the Eustachian tube. Provided mastoiditis can be excluded, these measures can be used without fear of serious risk for several weeks. If the discharge continues, referral is recommended, when removal of enlarged adenoids may be advised. Sometimes, enlarging a small perforation in the tympanic membrane under general anaesthetic (GA) improves the condition and provides an opportunity for suction removal of material from the middle ear. An irritating grommet suggested by granulation tissue should be removed under GA.
Figure 2.2 Massaging drops into the middle ear.
Rarely, continuing discharge may suggest that the mucosa throughout the mastoid air cell system has become muco-secretory in nature. This may be an indication for a cortical mastoidectomy.
The discharge is usually accompanied by itching and irritation. It is often thick and smelly, from infected wax and desquamating skin. The organisms are usually Gram negative. The ear drum, when exposed, is found to be normal, and there is no hearing loss. Examination of the drum head can be difficult because of meatal swelling and debris within it. Suction removal of dead material is needed, using a microscope, with particular attention to the anterior recess, where the meatus curves forward to make an acute angle with the drum beyond.
Chronic otitis externa is partly due to skin diseases – eczema, seborrhoeic dermatitis or psoriasis – and partly to external trauma to the ears from wetting, drying with a dirty towel or scratching.
Chronic otitis externa is treated by so-called aural toilet and the application of topical medication. Cleaning to remove infected debris must be performed under good illumination, using cotton wool on a wire wool carrier, or by suction under a microscope.
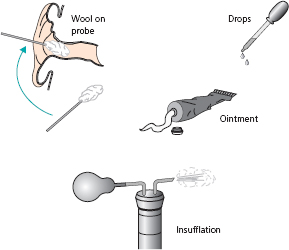
Toilet should be repeated, ideally every day. Microbial swabs for fungi as well as bacteria will guide the choice of topical applications, such as combinations of antibiotics like gentamicin and neomycin with a steroid. Fungal infections need antifungal agents such as nystatin or clotrimazole. Medication may be instilled as drops twice a day, painted on the meatal walls with cotton wool on a wire wool carrier, inserted on an impregnated gauze wick, or insufflated as a powder after toilet. Eczematous reactions of the pinna require application of antiallergic creams or ointments (Fig. 2.3).
Systemic antibiotics are never necessary. Topical preparations should not be used for long periods (7–10 days at most). There is, however, a case for applying drops intermittently (for example once a week) to try to prevent repeated relapses.
When intrinsic factors predominate, permanent cure rather than alleviation may be impossible. Subepithelial fibrosis can cause gross narrowing of the meatus, causing lack of ventilation and difficulties in performing adequate toilet. An operation to widen the meatus is then needed. All patients who have had chronic otitis externa must be warned to protect their ears from water and never poke cotton buds or other implements into the meatus.
There are two forms of chronic suppurative otitis media, which should be considered as distinct and separate entities. Both present with conductive deafness and discharge without pain. In both, discharge issues through a perforated drum; however, one is styled ‘safe’, while the other is ‘unsafe’, because of potentially serious complications (Fig. 2.4).
Figure 2.3 Applying medication to the external auditory meatus.
The safe variety (or active mucosal chronic otitis media) carries no serious risks. Disease affects the mucosa of the lower front part of the middle ear cleft (‘tubotympanic’). In contrast, the unsafe variety (active chronic with cholesteatoma) threatens the hazard of spread of infection intracranially. This disease is associated with erosion of surrounding bone. Cholesteatoma (described below) or chronic osteitis involves the upper back part of the middle ear cleft, and so anatomically it is described as ‘atticoantral’.
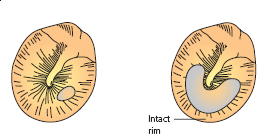
In the safe type, the perforation is ‘central’ (Fig. 2.5). By this, it is meant that no matter how large the defect, there is always a rim of drum or even just its annulus around the edge. It involves the vibrating part of the tympanic membrane – the pars tensa, below the malleolar folds, at the level of the lateral process of the malleus.
Figure 2.4 Two types of chronic suppurative otitis media.
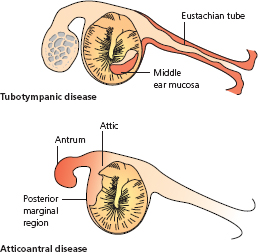
Figure 2.5 Central perforations.
The perforation in the unsafe variety extends into the very bony edge of the drum, where it produces chronic bone necrosis and is associated with the production of granulation tissue or a polyp. This so-called marginal perforation (Fig. 2.6) is usually posterior, or in the attic region of the drum head above the malleolar folds – the pars flaccida.
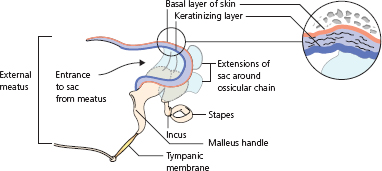
Discharge from the ‘safe’ variety arises from the inflamed and secreting mucosa of the middle ear and is copious, mucoid or mucopurulent. It may be intermittent. In the ‘unsafe’ variety the discharge is scanty, foul smelling and continuous. It comes from infected debris accumulating within a cholesteatoma sac (Fig. 2.7). Cholesteatoma is skin – stratified squamous keratinizing epithelium – that has invaded the middle ear cleft to form a cyst surrounding the ossicular contents of the attic, descending into the middle ear mesotympanum and extending back into the mastoid antrum and its connecting air cells. When the accumulating keratin within the cholesteatoma becomes infected, its outermost layer, which is the basal layer of the skin, develops a propensity to erode adjacent bone, threatening spread of infection beyond.
Figure 2.6 Marginal perforations.
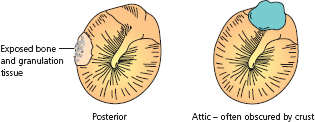
Figure 2.7 Cholesteatoma sac in attic.
The distinction between the two kinds of chronic suppurative otitis media is made by examining the ear drum after removing any discharge – ideally under an operating microscope and sometimes under anaesthetic. It is often impossible to make a certain and reliable distinction on a first inspection.
In safe ears, the aim is to eliminate discharge and possibly to assist hearing deficit. Drying is achieved by treating infection or allergy in the upper respiratory tract and by aural toilet to remove infected material. Antibiotic drops containing steroids are routinely useful.
Once the ear is dry, the state may be described as ‘inactive chronic otitis media’, and recurrent discharge may often be prevented by protecting the ear from water and by promptly treating upper respiratory tract infection, or by closing the defect in the ear drum surgically (myringoplasty). Hearing defects may, if necessary, be helped by using a hearing aid, or by reconstructing the drum and the ossicular chain (tympanoplasty).
An unsafe ear must be rendered harmless as the priority before considering tackling any hearing loss. The traditional approach is to remove diseased and infected bone and to fashion a smooth, wide cavity opening into a wide external ear canal. As the ear heals, the cavity becomes lined with skin, which is histologically identical to cholesteatoma but which excretes its dead squames easily to the exterior through wide access to the external ear canal. Operations are named according to the extent of bone removal, which is dictated by the extent of disease.
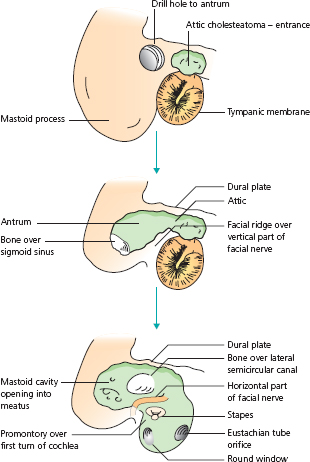
Radical mastoidectomy is one extreme of this kind of operation. The mastoid antrum is opened with a drill. As access to the antrum is enlarged, it is extended forward into the attic region of the middle ear. Removal of bone over the attic and antrum joins the mastoid cavity and middle ear into one. Diseased material is extirpated as the operation proceeds. All the ossicular chain except the stapes is removed. The cavity is made as hemispherical as possible, while respecting the safety of the adjacent facial nerve, labyrinth, sigmoid sinus and dura (Fig. 2.8). Lesser cavity operations, dictated by the disease limits, are called atticotomy, attico-antrostomy or modified radical mastoidectomy, depending on their extent. Parts of the ossicular chain and tympanic membrane may safely be preserved.
Figure 2.8 Right radical mastoidectomy.
All of these ‘open cavity’ operations are liable to repeated discharge, which may be provoked if their lining is exposed to ingress of water. Therefore swimming is to be avoided.
Fig. 2.9