American College of Obstetricians and Gynecologists. ACOG Technical Bulletins and Committee Opinions. Washington, D.C.: ACOG, 2004-2012.
Textbook of Gynecology. 2nd ed. Edited by L.J. Copeland. Philadelphia: W. B. Saunders Company, 1999.
Williams Obstetrics, 23rd ed. Edited by F. G. Cunningham et al. Norwalk, Conn.: Appleton and Lange, 2010.
THE WORKS • OVARIES • FALLOPIAN TUBES • UTERUS • CERVIX • VAGINA AND VULVA • BREASTS • THE BOSSES • PITUITARY • HYPOTHALAMUS • THE WORKING OF THE WORKS • MENSTRUATION • WHAT IS A NORMAL PERIOD? • KEEPING A MENSTRUAL CHART • MITTELSCHMERZ • WHEN A PERIOD BECOMES A QUESTION MARK • AMENORRHEA • OLIGOMENORRHEA • POLYMENORRHEA • DYSMENORRHEA • HEAVY BLEEDING AND CLOTS • REGULATION OF PERIODS • BIRTH CONTROL PILLS • DIAGNOSTIC PROCEDURES • PMS—FACTS AND FICTIONS • TO DOUCHE OR NOT TO DOUCHE • DOUCHING TO PREVENT PREGNANCY • PAINFUL INTERCOURSE • LUBRICATION • INFECTION • AGE •
The basic anatomy of the human female is a mystery to many women. Even highly educated and sophisticated women may not know the difference between a urethra and a ureter. A patient of mine, a lawyer, was surprised to learn that her fallopian tubes were not attached to her navel when we discussed the procedure of tubal ligation, that is, the tying and cutting of her tubes, after she delivered her third child. Let us attempt to clear up any possible confusion by taking a tour of the female reproductive organs.
THE WORKS
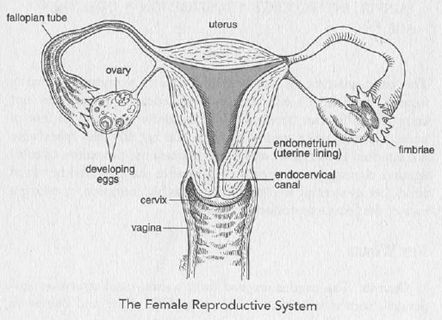
Ovaries. The ovaries are two firm, walnut-sized structures suspended from either side of the uterus. Dull white and bumpy in appearance, they produce the hormones estrogen and progesterone. Eggs are stored inside the ovaries, and every month, in a process called ovulation, one of the ovaries releases an egg, or ovum, the size of a sugar granule. First, an egg sac called a follicle develops inside the ovary in response to follicle-stimulating hormone (FSH), and when the follicle ruptures on command of certain other hormones, the egg is released.
A female is born with all the eggs she will ever have; no more will be produced in her lifetime. When a female fetus is twenty weeks old, the ovaries contain six million eggs. This is their peak number. By the time the baby girl is born, the number of eggs is already down to two million. By adolescence, 300,000 eggs remain, and when that girl becomes a 36-year-old woman, only 34,000 eggs remain. Luckily, women require no more than about 400 eggs throughout their entire reproductive lives, suggesting that the much, much larger number of eggs available is a fail-safe mechanism on the part of Mother Nature.
Fallopian Tubes. There are two fallopian tubes. Each extends from the top of the uterus to form a passageway for the egg to travel from the ovary to the uterus. Although usually pictured as standing out in a T formation from the uterus, the fallopian tubes actually droop behind the uterus, hanging in a limp fashion with fingerlike projections (fimbriae) at the ends. These fimbriae sweep over the surface of the ovaries at regular intervals, and when an egg is released from an ovary, the fimbriae on that side vacuum up the egg. The egg then travels down the fallopian tube into the uterus, where, if it has been fertilized, it is implanted.
If a patient of mine has difficulty envisioning the spatial relationship of the fallopian tubes to the uterus, I am apt to impersonate the two by standing with my arms hanging loosely behind me. My body then represents the uterus, my arms the fallopian tubes, and my fingers the fimbriae.
Uterus. Often referred to as the womb, the uterus is the "storage facility" for the fetus in a normal pregnancy. It is divided into two unequal parts, with the larger part being the body, or fundus, while the smaller is the cervix, or neck. The lining of the uterus, which is called the endometrium, undergoes change in accordance with changing levels of circulating hormones. Right after a menstrual period, the endometrium can be as thin as indoor-outdoor carpeting, while at midcycle it is as plushly luxuriant as a velvety Oriental rug. When this endometrial lining is sloughed off each month, the resulting blood flow is referred to as menstruation. As well as blood, the menstrual flow contains tiny fragments of shed uterine lining.
Cervix. The cervix is that part of the uterus (the neck) that is connected to the vagina. It feels like a bump at the top of the vagina and is as firm as a nose. The cervix produces mucus, and this mucus changes consistency in response to hormones, particularly estrogen. Just prior to ovulation the mucus is thin and elastic so as to allow sperm from the male easier access to the womb. At other times it is thick and less penetrable.
An internal os, or mouth, at one end of the cervix opens into the body of the uterus, and an external os at the opposite end opens into the vagina. These openings act like doors. After childbearing, the external os may remain ajar, but the internal os is characteristically closed. The corridor between the two is known as the endocervical canal, and it and the external os are important in gynecology because it is here that cell samples are collected for a Pap smear. The internal os, on the other hand, is important in obstetrics because a mucus plug in this area prevents bacteria from ascending into the womb and infecting the fetus.
Vagina and Vulva. The vagina is a tubular structure linking the uterus to the outside world of the vulva. It accommodates the male organ during intercourse, and during childbirth it is the birth canal through which the baby enters the world. In the young female, before intercourse has occurred, the entrance of the vagina is partially covered by a membrane called the hymen. Initial intercourse tears the hymen, leaving tags of tissue behind. Because the tearing is rather like a fist going through a bass drum, the process can be painful and bleeding usually occurs.
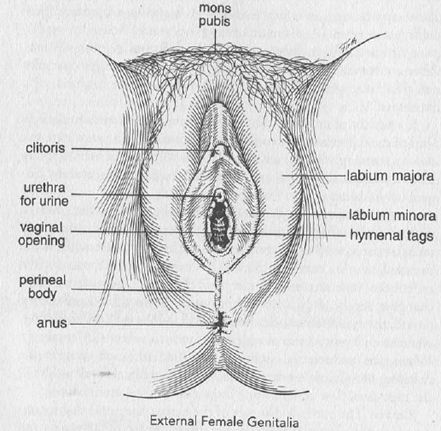
The vulva includes all structures visible on the outside, from the fat-filled cushion covering the pubic bone, known as the mons pubis, to the anus. The external female genitalia include the clitoris, the labia majora (labium majus) and labia minora (labium minus), and the urethra. The labia, plural from the Latin word for "lips," are the inner and outer folds of skin enclosing the clitoris, urethra, vagina, and the perineal body, which is the area between the vagina and the anus.
When a woman is lying on her back, uppermost is the clitoris, which is analogous to the penis in the male and is the prime organ of sexual sensation and pleasure. Next comes the urethra through which urine flows from the bladder to the outside. Just below the urethra is the vagina, and the last opening farther down is the anus. Figure 2 shows why it is important, after urinating, to wipe from the front to the back rather than the reverse; the anus is filled with bacteria that can cause a bladder infection if allowed to gain entry through the urethra.
Breasts. The breasts are mammary (milk-producing) glands responsive to hormones released during the monthly cycle and after childbirth. When the breasts are producing milk, this process is called lactation.
THE BOSSES
The breasts, ovaries, and uterus are referred to as end-organs, that is, their workings are dictated by chemical messengers coming from other organs, in this case the pituitary gland and the hypothalamus, both of which are situated in the head.
Pituitary. The pituitary gland is an endocrine organ, that is, an organ that secrets substances into the blood which have a specific effect on other organs. The larger part of the pituitary, the anterior lobe, comes from the same tissue as the pharynx, which is the tube connecting the mouth and the esophagus. The smaller part, the posterior lobe, is formed from the floor of the hypothalamus in the brain. It sits immediately beneath the brain and is connected to it by a stalk.
The pituitary secretes follicle-stimulating hormone (FSH) in response to low or declining levels of circulating estrogen and progesterone. The FSH stimulates egg follicles to grow and compete to become the large follicle holding the egg that will be released from the ovary at midcycle (ovulation). As midcycle approaches, the level of estrogen increases, which in turn shuts off FSH and prompts a rise in another pituitary hormone, luteinizing hormone (LH). This hormone stimulates release of the egg from the ovary, usually at mid-cycle. The ruptured follicle left behind is called the corpus luteum (yellow body). This corpus luteum secretes a hormone called progesterone. Progesterone, in concert with estrogen, prepares the uterine lining to nourish the fertilized egg. If the egg is not fertilized, the corpus luteum degenerates over the next 14 days, a process that both signals the uterine lining to slough off (menstruation) and triggers a rise in the level of FSH, and the whole cycle starts over again.
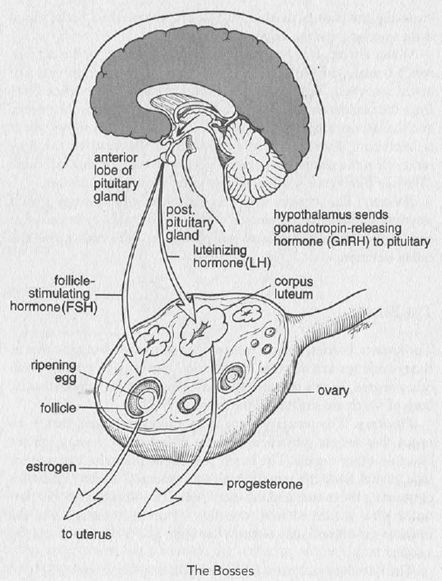
Hypothalamus. This organ, situated in the brain, is the ultimate boss. It produces gonadotropin-releasing hormone (GnRH), which stimulates the pituitary to release FSH and LH, and these in turn stimulate the production of estrogen and progesterone by the ovaries.
THE WORKING OF THE WORKS
In young girls the first signs of maturation occur in the nipples and breast tissue. This stage is called the thelarche, from the Greek word for nipple. Sometimes as early as six years of age but usually around ten, girls start developing little mounds on their chest, and mothers who observe these "mosquito bites" note to themselves that the menarche, the establishment of menstruation, cannot be too far off. An intermediate stage comes before the menarche, however. Known as the pubarche, this stage occurs about a year after breast tissue begins to develop and is characterized by the appearance of hair in the pubic area and under the arms. It is another year or so after this that menstruation commences.
Menstruation. The average age of the onset of menstruation is 12.6 to 12.8 years, with the range being from 9.1 to 17.7 years. Mothers tell me about daughters going on 11 who expect to have their periods by the time they are 12. The day after their twelfth birthday they are saying, "Mommy, Mommy, Joanie has her period. How come I don't have mine?" What they don't realize is that 12 years and 8 months is almost 13 years and they are jumping the gun a bit. But I must admit this is preferable to earlier times when mothers were too reticent to prepare their daughters for what was coming. All too many girls, out climbing trees with their brothers, suddenly feared they were bleeding to death and entered womanhood on a shock wave of dismay.
Some girls who are thin do not have their periods until they have reached a critical body weight, others not until they are 16 or even 18 years old. Although these ages are still within the normal range, albeit at the upper limit, either peer pressure or a nervous mother is likely to have landed the girl in a gynecologist's office by the time she is 14 or 15. The advice she receives then will probably be to wait and see. Only when absolutely nothing has happened by age 16 does the possibility of a hormonal problem need to be investigated.
What Is a Normal Period? Periods (menses) are irregular in 50 percent of adolescent girls. A period may come once and then not again for another six months, or come once every three months, or skip back and forth between once a month and once every two or three months. Bleeding may be light one month and heavy the next, and it may last for two days or five days. All sorts of variations from what adult women experience as normal are common because it can take time for the hormones to become regulated. But eventually they do settle down and a pattern is established.
The normal cycle is said to be 28 days, the length of the lunar (not the calendar) month, but variations on "normal" are legion. Seldom in my experience as a gynecologist have I encountered a person with a 28-day cycle. I am much more used to hearing 30 days, 26 days, 40 days, even once every two months or, rarely, three months.
“Normal," then, is what is normal for the particular individual. After the hormones have settled down and the periods are coming regularly, whether the pattern is every 28 days, every 40 days, or every two months, when it has persisted for a couple of years, it is clear that is that particular female's cycle; it is normal for her.
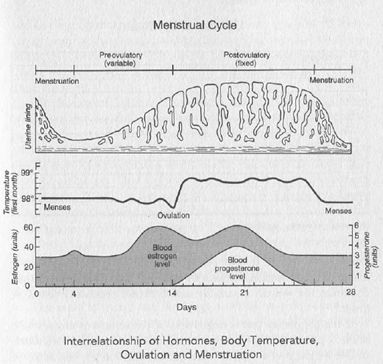
If the cycle is longer than 28 days, the variation in time comes prior to ovulation because after ovulation occurs, it is always, in every woman, 13 to 15 days until the start of the next period. With a 28-day cycle, 14 days will be preovulatory; with a 40-day cycle, 26 of those days will be preovulatory. This is important to know if pregnancy is desired, as I found out when I wanted to get pregnant; I had a 40-day cycle, so I was ovulating on day 26, not on day 14 as the textbooks have it.
Keeping a Menstrual Chart. Not only is there variation in cyclicity among women, but the timing of cycles does not necessarily remain the same throughout the 35 to 40 years a woman menstruates. A woman in her 20's may menstruate every 32 days, then she enters her 30's and her periods come every 26 days, and after 35 she may go to 40 days. Although the change should be investigated, if a new regularity becomes established, then it is clear that a new phase has been entered.
A woman herself is her own best control, that is, she should compare herself with herself. What matters after a pattern has been established is whether there is any change in it. To this end, every female, when she starts menstruating, should keep a chart. The type illustrated below works well because marking the squares to indicate a period allows any deviation in timing to become immediately apparent.
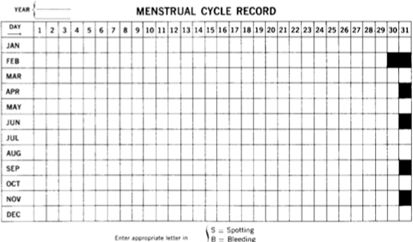
When a woman comes to me with a report of menstrual irregularities, I say, "Let's look at your menstrual calendar. Okay, it was every 26 days up till here, and then what happened?"
She may answer, "That's about the time I started horseback riding." Or "I wanted to lose weight and went on a near-starvation diet." Or "I fell in love and began having intercourse." Any one of these can be a sufficient explanation—but only after other possible causes have been ruled out in a process known as diagnosis by exclusion.
If I see from her calendar that 40 days have gone by, pregnancy is the first possibility to be excluded. I ask the woman if she is sexually active, and I explain that "sexually active" means any exposure to sperm. It does not have to be complete intercourse. It can be "just outside, he didn't come in." If by this or any other definition the woman is sexually active, then a pregnancy test is in order.
If the pregnancy test is negative or if the woman is not sexually active, I proceed to rule out other possible causes, such as a sudden sizable weight gain or loss or a marked increased in physical activity, such as going into training as a runner or starting medical school. When no such explanation exists, I suggest to the woman that our best course is to wait for another cycle to see whether a change in periodicity is establishing itself.
"You're 30 now," I say. "When you're 35, it may change again." Although this change in periodicity is not described in textbooks, I have seen it over and over in my practice, so frequently that it cannot be abnormal. As far as I am aware, no studies have been done, no statistics gathered, perhaps because nobody thinks it worth bothering about, but I know from my own experience that a lengthening or shortening of the cycle often occurs, and I have the impression that the ages ending in zero or five—20, 25, 30, 35, 40—seem to be involved most often.
Having this bit of information does not mean, however, that a woman should shrug off a deviation in her cycle. While it is likely to have a benign explanation, any change in cyclicity should send a woman to her gynecologist promptly. This is why keeping a menstrual chart is important: It acts as an early warning system for the woman, alerting her to seek medical attention, and it is a visual aid for the doctor that is far more informative than a vague statement such as, "My periods seem to be getting more frequent."
Mittelschmerz. Another advantage of keeping a menstrual chart is that it identifies the time of ovulation, which occurs at the mid-point of the cycle. When the egg ruptures through the ovary, there can be an imbalance in estrogen and progesterone levels, and that may in turn affect the lining of the uterus, causing it to slough off a little bit of blood. This slight discharge is known as mittelschmerz, German for "a pain in the middle," although it is more graphic to think of it as a "schmear in the middle."
When an anxious patient says, "I'm bleeding every other day now," and I ask her when it started and she answers, "October fourteenth," if I look at her menstrual calendar and find that October 14 is right at midcycle, I am relieved. I know it is mittelschmerz and nothing to be concerned about.
The same is true if the discharge is white or pale yellow. The vagina as well as the uterus may respond to the midcycle surge in hormones with an increased discharge. Patients come to my office complaining, "Oh, the discharge is so heavy. Something must be terribly wrong." I ask for the date of the first day of their last period, and if the discharge is particularly noticeable at midcycle, I reassure them that it is not something to be concerned about. "I'll take a culture," I say, "to make sure it's not chlamydia and not infectious, but nine chances out of ten it's only mittelschmerz."
WHEN A PERIOD BECOMES A QUESTION MARK
Amenorrhea. There is primary amenorrhea, which is no periods at all by age 16, and secondary amenorrhea, which is cessation of already established menses, the latter being by far the most common. If the periods have ceased and the patient is not pregnant, a hormonal imbalance is the most likely explanation. If the patient is an adolescent, I inquire into whether she has been losing weight or is distressed. Usually it turns out that she has been on a diet and lost 35 pounds, or she has gone away to boarding school for the first time, or her parents are in the midst of a divorce and there is a great deal of stress in her life.
Stress can cause the periods to cease in adults as well as adolescents. But amenorrhea should not be assumed to be due to stress without a physical examination to eliminate other causes. Nor should the amenorrhea be allowed to go beyond three months because when the woman finally does have her period, it is likely to be a dangerously heavy bleed. Estrogen has been affecting the lining of the uterus, making the endometrium nice and plump, and those growing cells need to be sloughed off. When they are not, when the uterus has been stimulated for so long without shedding, the woman may end up in the hospital with a hemorrhage.
Oligomenorrhea. While amenorrhea is the absence of menses, oligomenorrhea is defined as abnormally infrequent or scanty menstruation, and the same considerations apply. It must be medically evaluated to try to pin down the cause, and steps must be taken to correct it to obviate the risk of the growing cells piling up in die uterine lining.
Oligomenorrhea followed by amenorrhea for several months in a woman in her late 40's is usually the first sign that she is entering menopause.
Polymenorrhea. At the opposite extreme is the situation where periods are coming every two to three weeks. This type of irregular bleeding, be it in an adolescent, a 25-year-old, or a 55-year-old, must be evaluated promptly to rule out polyps or any other abnormal condition that may be causing the polymenorrhea. When the uterine tissue has been biopsied and found to be normal, then we assume the dysfunction has to do with hormonal regulation. But we cannot then go on to say that the cause is an overactive or underactive pituitary gland or some other imbalance because the truth is that we do not know. The old term for polymenorrhea was dysfunctional uterine bleeding, but that was just a more high-sounding way of saying the cause is unknown.
Dysmenorrhea. Dysmenorrhea, or cramps, is colicky pain or discomfort in the mid or lower abdomen, perhaps radiating to the lower back and legs, experienced with a period. The cause of cramps is thought to be contractions of the uterus as the lining is being sloughed off, with the contractions being a direct effect of prostaglandin on the uterine muscle. (Prostaglandin, present in the uterine lining, is a substance that causes muscle contractions.) Although most women have cramping during their menses, the abdominal symptoms are usually mild and subside within a few days after the beginning of the menstrual flow. If this is not the case and the cramps progress to severe or unrelenting pain, the term dysmenorrhea is applied and the condition calls for medical evaluation and treatment. The nonsteroidal anti-inflammatory drugs such as aspirin, ibuprofen, naprosyn, and mefenamic acid (Ponstel) block the prostaglandins from exerting their cramping effect and provide relief of mild to severe menstrual cramps.
Menorrhagia (Heavy Bleeding). Even though the menses feels as if it is opening the gates of the Red Sea, when scientifically measured, the average amount of blood lost during normal menses (lasting from 1 to 8 days) is only between one and five tablespoonsful. For some women, it feels as if she is losing more like a cup of blood a day during the first days of her menses. However, when the blood loss is greater than 5 tablespoonsful (80 cc.), it is considered to be heavy menstrual flow or menorrhagia. A new treatment for heavy menstrual flow was recently approved by the Food and Drug Administration in November of 2009. It is the first non-hormonal treatment for heavy menstrual bleeding, especially bleeding associated with myomas (fibroids). The medication is tranexamic acid (Lysteda). It is an antifibrinolytic drug, which means it interferes with the body’s ability to breakdown blood clots and therefore, reduces blood loss. The downside to this drug is that it may increase the risk of developing blood clots and deep vein thrombosis. However, studies have shown no difference in the incidence of blood clots between women using Lysteda compared to those not using Lysteda.
Clots. A patient will arrive at my office thoroughly upset because "My period's coming out in clots." I ask how big the clots are, and if she tells me they are anything smaller than a piece of liver and are not soaking an external pad in an hour, I tell her not to worry about them. I explain that the endometrial lining tissue of the uterus gets plush and succulent and thick under the influence of estrogen. If progesterone is not secreted in timely fashion to counteract the estrogen, the lining continues to thicken and may start breaking off in pieces. The longer the time between periods, the more likely this is to occur, which is why progesterone is often prescribed for patients whose periods are delayed or widely spaced to stabilize the endometrium and ensure that the bleed will be orderly.
Even in a normal period there will be blood clots because it is vascular tissue that is being shed, but the actual pieces of endometrium tend to be microscopic and most women do not notice them. Since they are particularly likely to emerge when the toilet is being used, they are simply flushed away. New pads will sometimes show bits of clot; if the pads have webbing on the outside, some tissue may remain on top while the blood soaks through to the layers beneath. The only time to be concerned about clots is when excessive bleeding soaks an external pad with bright red blood and the pad needs to be changed every hour.
REGULATION OF PERIODS
Birth Control Pills. Many gynecologists prescribe birth control pills for women with polymenorrhea on the theory that the steady supply of estrogen and progesterone the pills provide will make up for any hormonal imbalance. A course of low-dose birth control pills stabilizes the endometrial lining and allows it to build up. The pills are used for three to six months; after they are discontinued, the periods usually respond by coming regularly again.
It is a different story, however, if, in an attempt to regulate her cycle, birth control pills are prescribed for the woman whose periods come only every two or three months. Obviously, the hypothalamus and pituitary with their control mechanisms for the period are not functioning at 100 percent. They may be functioning at 85 percent, which is not a problem; it only means that the period comes every eight weeks instead of every four. However, many doctors feel that a woman must have a period every 28 days and prescribe birth control pills to make certain she does.
The woman dutifully follows a regimen of 21 hormone pills a month and the pills take over the prerogatives of the hypothalamus and pituitary, in effect putting them to sleep. Now it is the birth control pills that are dictating the cycle, causing an artificial period, and when the woman stops taking them after six months or so, she may never have a period again.
I have had any number of women come to my office saying, "I was having periods every two months and my gynecologist wanted to ‘regulate’ me so he put me on the Pill. I took it for a year and then I stopped because I want to have a baby, and now my periods don't come at all." I explain that the little pituitary and hypothalamus glands that were struggling along every two months got sat on by the big Pill and now cannot get themselves cranked up again. (For the treatment of anovulatory cycles, see Chapter 7.)
Conversely, some patients with perfectly normal monthly menses do not want to be inconvenienced by having a period each month and have resorted to taking birth control pills for an extended period of time, i.e., for three months continuously, in order for their menses to come four times a year. Well, that may sound good but it is not good and sound. Without a monthly period, a patient may not know she is pregnant. Moreover, the original studies on oral contraceptives were performed with a week hiatus of taking inactive pills for seven days followed by taking active hormones for twenty-one consecutive days. The risk of stroke, blood clots, and other maladies have not been studied extensively regarding the continuous use of oral birth control pills for three months and this new paradigm may also increase the risk for developing side effects, such as irregular bleeding. After all, they are hormones. However, those patients who have been diagnosed with endometriosis should consider delaying menses for an extended period of time by the use of this three-month birth control pill regimen because it is medically indicated and the benefit in managing her endometriosis far outweighs the risk.
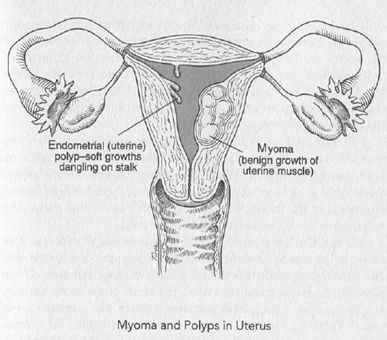
Diagnostic Procedures. Heavy or irregular bleeding (menorrhagia), periods that are coming without rhyme or reason, warrant careful investigation. A sonohysterogram (an imaging study using transvaginal sonography and saline solution instilled into the uterine cavity) is one way of evaluating the cavity for polyps or other abnormalities. Another modality for attempting to find out the cause of abnormal bleeding, especially in post-menopausal patients, is by means of an endometrial biopsy. This can be done in the gynecologist's office. A scoop-shaped plastic catheter called a curette is inserted into the uterus to scrape off a sample of the endometrial lining. With training and experience the gynecologist becomes skilled at judging the feel of the endometrial cavity, whether it is irregular or jagged, whether there are things like polyps growing in there or whether the lining is clumped to one side. Sometimes a polyp comes out in the sampling pass made with the curette, or a polyp may be hanging outside the cervix like a tongue and the gynecologist can just grasp it and remove it.
The tissue removed is sent to a pathology laboratory for examination.
A concern with endometrial sampling is that the gynecologist may be taking a sample on the right side of the uterus, for instance, and missing cancerous changes on the left; but if malignancy is present, it is usually throughout the uterus, and in general, office biopsies are very good at providing a diagnosis. Sometimes they even prove remedial: The pass with the curette smoothes the endometrial lining or removes the polyp, and the irregular bleeding ceases. However, if the procedure yields no results or inconclusive results, a formal D and C—dilatation and curettage of the uterus—is the next step. The patient often protests, "Why didn't you do that in the first place?" My answer is that I want to see if I can obtain a diagnosis without having to resort to a more involved procedure. Even though a D and C is probably the most frequently performed of all operative procedures and is viewed as routine, I consider that whenever a patient goes to the operating room, there is always the potential, however slight, of a mishap. In a D and C there can be perforation of the uterus or complications from the anesthesia, and I prefer to avoid the risk if I can get the same information from an office procedure.
If heavy bleeding continues despite the office procedure, one polyp may have been removed but another missed, or the lining of the uterus is clumped to one side, or a submucous myoma has indented the lining. Most myomas grow on the outside of the uterus like Mickey Mouse ears, but some grow inside, making the endometrial lining irregular and causing a disruption in the menstrual sloughing-off process (see chapter 16).
A D and C is done in the hospital in a same-day procedure—in by nine, out by five, like dry cleaning. It is done under heavy sedation or light general anesthesia. When the patient regains consciousness, she is likely to be experiencing cramps because there has been instrumentation in the uterus, but medication will ameliorate them. She will need someone, however, to escort her home.
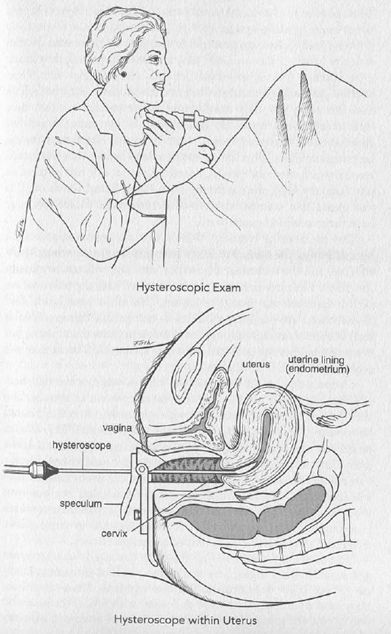
A D and C is designed to be both diagnostic and therapeutic. The cervix is first dilated (stretched) in order to accommodate the curette, and curettage smoothes the lining, making it clean and even. If the physician finds it necessary to inspect the inside of the uterus visually, a hysteroscope—a long, thin instrument much like a telescope—is used. When the presence of a myoma is noted within the uterine cavity, a more sophisticated and involved procedure than a D and C is carried out at a later date, or if the tissue obtained is diagnosed as malignant on laboratory examination, the patient will be referred to a cancer specialist.
PMS—FACTS AND FICTIONS
At midcycle there is a sudden surge in hormonal release because the body is getting ready for pregnancy. If the egg is fertilized, large amounts of hormones are needed to support the base mechanism of the growing placenta, but if the egg is not fertilized, the woman is stuck with the excess hormones and PMS, or premenstrual syndrome, is the result. Women respond to it in different ways: Some get bloated, some experience supercharged emotions, some erupt in acne because they have receptors for the hormones in their faces. There is even a rare condition called catamenial pneumothorax in which receptors in the lungs respond to the surge of hormones and blood vessels rupture, causing breathing difficulties. The woman who knows that her body responds to the hormone surge in this way learns to take it in stride. After the initial "Eek!" she says, "Oh, it's just my lung again. It's midcycle."
Some women have no perceptible reaction. Of those who do, the majority handle it the same way they handle their period; they know it is coming and adjust their activities accordingly. But some women—not a large number—become emotionally disturbed and are diagnosed with premenstrual dysphoric disorder (PMDD), which is a severe form of PMS. The symptoms of PMDD are similar to those of PMS, but are severe enough to interfere with work, social activities and relationships. This does not mean that their hormone release is greater but that they react more sensitively to it. If a woman is by nature somewhat depressive or somewhat manic, what is already there as a matrix becomes amplified. This leads some people to believe that all women are crazy or have mood swings, but this is not so, nor is it justified to say, "Oh, my God, she's suffering from PMS. Better watch out." It just means that women who are borderline manic-depressive may have their condition exacerbated.
The problem in treating PMS is that the symptoms are not necessarily all the same. Ms. X can have one set of symptoms, Ms. Y another, and the treatment that works with one will not work with the other. The physician who grows frustrated with the failure of his or her approach may resort to saying, "It's all in your head." But women need not—indeed, should not—accept this dictum. PMS and PMDD are real. They exist. PMS is more prominent in some patients than others, but every woman has the potential of having severe PMS because of the physiologic surge in hormones.
I suspect that how a woman copes with it, whether she tells herself that she knows it is coming and just rides it out or whether she uses it as an excuse, depends somewhat on her mindset. But I could be wrong. There are still a lot of unknowns about PMS. We as physicians are placed in the position of being expected to know everything, and people do not like to accept that we do not—nor, for that matter, do some physicians. Patients look to us for answers, but sometimes we have to give advice based on nothing but our own experience, not on studies or investigations or experiments—which is certainly true in the case of PMS, where there is no single classic treatment approach to a classic set of symptoms.
The customary advice is: Get the sleep you need—at least seven and a half hours a night. Stay away from stressful situations. Don't eat refined sugar or chocolate. Exercise regularly. Know your own body, and try to formulate ways of dealing with PMS because if you don't, you are going to be debilitated for one week out of every month for 35 years. This counsel is not much consolation for the woman whose breasts and nipples become so sensitive that she cannot wear a sweater and would prefer not to have to answer the phone. But it is the best we can offer. Some patients may require anti-depressants.
One patient to whom I said something of this nature startled me by bursting out, "Gee, I hate female impersonators! If a man is going to impersonate a woman, he should have PMS, cramps, bleeding—he should have everything I go through before he has a right to dress up, put on makeup, and look pretty. It's not fair!" She had a point. But, then, whoever said life was fair?
TO DOUCHE OR NOT TO DOUCHE
Although this archaic ritual is being used less and less in contemporary time, an axiom handed down from mother to daughter through the ages is that females have to douche; to keep clean, they must douche after menstruation and after intercourse. When I ask older women their views on this, ninety-nine out of a hundred answer, "Oh, I have to douche. Definitely. I gotta." When I ask why, they say, "Because I've always done it, my mother's always done it, my grandmother's always done it." Douching is entrenched in female mores, perhaps in response to the ancient Biblical stigma of women being unclean, and despite any number of conclusive studies, women still carry on with this archaic, antiquated, and potentially dangerous procedure.
Nobody tells them that douching is unnecessary and harmful, certainly not the manufacturer who prospers financially by selling douche products. The only hope is for women to rise up and say, "What are we doing to ourselves? Let's question this." Douching should be like tonsillectomies. There was a time when every child had a tonsillectomy, until finally people said, "Wait a minute. Why are we doing this?" Sure enough, when studies were done, it turned out that every kid did not need a tonsillectomy. It is time we learned the same thing about douching.
When a patient says she douches "to make myself feel better, cleaner," I ask, "Is there an odor or something that makes you feel you have to douche?"
"No, it's just that when my period is over, I want to rinse out whatever is left there."
"That's logical, but do you know that your body does that? That's why you change your panties every day and throw them away after a while—because of a discharge, a natural discharge."
Bodies function excellently to take care of themselves. When menstruation ends, the 23 kinds of bacteria that are normally present in the vagina do the cleaning up. Just like the bacteria in the mouth and in the rectum, they are there for a reason: to keep the area tidy and ride herd on invaders. Furthermore, in the average woman the pH of the vagina is four. The pH of the stomach is one because of the hydrochloric acid in it, the pH of water is seven, so the pH of the vagina is in the middle, slightly on the acidic side, where it needs to remain in order to provide the right environment for the cleansing bacteria. With douching, that natural balance is disrupted. The vagina has to try to repair itself and get back to that pH of four, and the bacteria that have been washed out by the douching have to try to grow and reestablish themselves; sometimes, before that can happen, fungus starts to move in.
Fungus, or yeast, is not bacteria. In fact, it is the bacteria that keep fungus under control. Erase the bacteria by douching and all of a sudden the fungus is saying, "Hey, fellas, come on in. There's nobody here." And more and more fungus moves into the vagina and happily multiplies. What does fungus do? It causes a tremendous itch and a tremendous discharge, and the woman is quickly going out of her mind. Thinking it will help, she douches again, and the three or four little bacteria that were trying to grow and reestablish themselves are washed out, leaving the field entirely to the fungus.
We women think we are being clean but actually we are causing problems by interfering with the natural environment and encouraging fungal growth. The normal balance of bacteria in the vagina is there to keep an acid pH level of four. If the pH tips to the alkaline side, fungus starts to move in. Many women believe that because vinegar is acid, douching with vinegar will preserve a pH of four, but they are not douching with vinegar; they are adding a little bit of vinegar to water, which has a pH of seven, and the result is not the same as preserving the natural pH of four.
The only way to get rid of fungal growth is with antifungal medications—but not over-the-counter preparations because they may encourage the emergence of different strains of fungus. Rather than trying to treat yourself, see your gynecologist. Better still, do not douche in the first place. If you have a malodorous discharge, again, see your gynecologist. Perhaps there is an overgrowth of a particular bacteria or perhaps you have picked up a venereal infection. Whatever it is, you will have a better chance of getting it remedied quickly than the woman who tries to deal with the discharge herself and waits a couple of months before seeking professional help. By that time the evidence is lost, and the gynecologist is doing culture after culture trying to identify the offending organism. On the other hand, walk into the gynecologist's office, say "I have this bad odor," and boom! there's your organism, that's it, we can take care of it. (See chapter 18.)
If women did not douche, I venture to say that it would save millions of dollars in gynecologic visits. Months of suboptimum treatment with home remedies so obscure what the original problem was that just about the best the doctor can do is to try one thing, and if that does not work, try another, and then a third and a fourth; and the poor patient has to keep coming back and back and back.
As well as the problem of an invasion of fungus, there is the possibility of causing pelvic inflammatory disease by douching. The vagina with its bacteria is separated from the uterus by the cervix, and the uterus is sterile. Use a douche and the bacteria safely in their hometown of the vagina may suddenly be picked up and flushed into the uterus, where they have no business being and where they can cause infection. The infection may damage the fallopian tubes and increase the chance of an ectopic pregnancy, "ectopic" meaning "out of the normal place."
Forget the folklore that says women have to run to the bathroom and douche every time they have intercourse. The vagina is open-ended and most of the semen drains out. When you stand up, it is out of there, and any remnant left behind is quickly whipped away by the bacteria in the vagina.
One of my female professors in medical school used to say this: "Do you douche your eyes? Do you douche your nose? Then why are you douching your vagina? The body has a way of taking care of the eyes and nose, and it has a way of taking care of the vagina, a natural way of renewal, of keeping everything balanced, of making sure that no offending organisms will cause problems. Interfere with the natural balance and you are asking for trouble. In short, the only thing that should go in a vagina is a penis, the only thing that should come out is a baby."
Unfortunately, patients, when they have a recurrence of symptoms, treat themselves with over-the-counter creams and because of overuse, strains of fungus not susceptible to anti-fungal medications are appearing. As it becomes more and more difficult to treat vaginitis successfully, it is even more imperative that douching be avoided because douching is likely to be the prime cause. Contrary to rumor, vaginal infections are not picked up from toilet seats. If any personal area is at risk from a toilet seat, it is the external vulva, not the internal vagina. The vulva can get lesions from picking up something on the seat, but bacteria need a warm, moist area to grow, and toilet seats, unless you knock somebody off real quick and take her place, are usually cold and inhospitable to bacteria.
Swimming pools may be warm and moist, but chlorinated water kills anything. Lakes are a bit more problematic; microorganisms or parasites in the water can get in the vagina, but the risk is not very great. As for baths, some water may enter the vagina, but the angle of the vagina is such that when you stand up, it flows out, and less water enters than in a douche because the walls of the vagina meet when it is empty.
Actually, baths are a good idea—that is, if they are solitary baths, not baths in a communal hot tub, which can indeed spread infection. If women took baths rather than showers, many of the problems they have in the perineal area—the region between the thighs—would be obviated. It is here, in the pubic hair and on the vulva, that perspiration and moisture can encourage the growth of fungus and bacteria. It is a pity that bidets have never become popular in this country. If women used bidets and/or took baths instead of showers, vaginal and vulvar irritations would occur considerably less often.
Douching to Prevent Pregnancy. I know it sounds ridiculous, but some women still use douching to try to prevent conception. The problem is that it does not work. With the woman lying down, when the man ejaculates, the semen is deposited at the top of the vagina in a pool under the cervix, and with the woman's orgasm, the cervix dips down into the pool and siphons up the ejaculate. Even without orgasm, the semen can enter the cervix like seepage from a pond and travel from there to the uterus. If the woman gets up and douches, no matter how quick she is, the sperm are quicker. By the time she douches, it is already too late. The sperm are on their way.
There does not even have to be an ejaculate. In the clear fluid on the tip of the penis before ejaculation, several hundred sperm are present. Patients say to me, "We didn't do anything, Dr. Thornton. All we did is just that he was very close." I have to tell them, "That's all it takes. The little buggers go, 'Oh, vagina? Thanks!' and Bingo! you are pregnant." The ovum is fertilizable only for 24 hours, but sperm can last five to seven days in the vagina, hanging around waiting for that egg to come out. The fact of the matter is that we are made to have offspring. Mother Nature set it up that way. Egg and sperm are going to get together if they possibly can, and douching is unlikely to stand in their way.
At the opposite extreme, douching can impact upon a woman's fertility in the future. It may make it impossible for her to conceive because douching has moved bacteria where they have no business being and they have caused pelvic inflammatory disease. The fallopian tubes become infected, and their cilia, the lashlike processes as fine as hairs that propel the egg toward the uterus, become club-like. It is as though the cilia develop arthritis and are no longer able to undulate, and without their flowing ripple to move the egg along, pregnancy is not going to happen. At least, it is not going to happen by the normal route; fertility specialists can bypass the tubes and plant a fertilized egg directly in the uterus; although this procedure does not always lead to a successful pregnancy. (See chapter 7.)
PAINFUL INTERCOURSE
Lubrication. Intercourse, coitus, and pareunia, which comes from the Greek word for "bedfellow," all mean the same thing. Dyspareunia, then, is the medical term for painful intercourse. So that my patients remember it, I sometimes joke that dyspareunia is better than no pareunia at all. Dyspareunia can affect a woman at any age, from the start of her sexual life into her seventies and eighties. The more sexually active a woman is, the less likely she is to experience it, while it is most apt to occur in someone who has been widowed and has not had intercourse for an extended period of time. When a widow finally finds a gentleman who makes her heart beat a little faster and one thing leads to another, that is when I get the phone call: "Dr. Thornton, oh my goodness …"
The source of the problem is that her vagina is not well lubricated, for lubrication is the key to pleasurable intercourse. Lubrication can be either natural or artificial, or some of both—that is, with some artificial augmentation of the natural lubrication that comes from the two Bartholin glands on either side of the vaginal opening. Natural lubrication does not require any discussion because the body knows exactly what to do, but when the body is not secreting enough lubrication, then augmentation with a sterile lubricant is in order.
Vaseline should never, ever be used for lubrication during intercourse. I cannot put the point too strongly because it is a longstanding myth that petroleum jelly is the answer to lubrication. It is not. It is an occlusive substance. It suffocates the pores in die perineal area, preventing them from contributing any natural lubrication at all and simply making matters worse. What is needed is a water-soluble lubricant, such as Surgilube, Astroglide, or Replens, any one of which aids immeasurably in the ability to have nonpainful intercourse.
These newer lubricants are like spinnbarkeit, a naturally occurring mucus produced by the cervix at midcycle. Just before ovulation the cervical mucus becomes very thin and elastic. If a gynecologist wants to know whether a woman has ovulated yet, he or she picks up a little mucus on an instrument and spreads the instrument apart. If the mucus stretches and stretches and is seemingly infinitely elastic, ovulation has not occurred. If, on the contrary, it is thick and sticky, then ovulation has occurred. Like spinnbarkeit, the newer vaginal lubricants now on the market are elastic and slick, as slick as oil on a road, and women who have had a problem with insufficient lubrication love them.
Age. A third possible cause is, simply, age. With age comes a thinning of the vaginal epithelium, and that leads to severe dyspareunia in some postmenopausal women. Treatment is an estrogen cream, applied vaginally, that builds up the vaginal wall. Because the estrogen in the cream is absorbed as rapidly as from a pill taken orally, women must also take progesterone in order to avoid an increased risk of uterine cancer. The progesterone may cause some spotting—a withdrawal bleed after the progesterone dosage is finished—but often it does not. In any event, the progesterone is needed so that the effect of estrogen on the uterus does not go unopposed. The exception is the woman who has had a hysterectomy; she can use just the cream as long and as often as she wishes.
Infection. Another source of dyspareunia can be infection, such as herpes, and what is termed nonspecific vaginitis or bacterial vaginosis (BV). Identification and treatment of the responsible organism take care of the problem.