
Copyright © Keith Souter, 2015
Illustrations © Keith Souter
All rights reserved.
No part of this book may be reproduced by any means, nor transmitted, nor translated into a machine language, without the written permission of the publishers.
Keith Souter has asserted his right to be identified as the author of this work in accordance with sections 77 and 78 of the Copyright, Designs and Patents Act 1988.
Condition of Sale
This book is sold subject to the condition that it shall not, by way of trade or otherwise, be lent, re-sold, hired out or otherwise circulated in any form of binding or cover other than that in which it is published and without a similar condition including this condition being imposed on the subsequent purchaser.
Vie Books is an imprint of Summersdale Publishers Ltd
Summersdale Publishers Ltd
46 West Street
Chichester
West Sussex
PO19 1RP
UK
www.summersdale.com
Printed and bound by CPI Group (UK) Ltd, Croydon, CR0 4YY
eISBN: 978-1-78372-577-9
Substantial discounts on bulk quantities of Summersdale books are available to corporations, professional associations and other organisations. For details contact Nicky Douglas by telephone: +44 (0) 1243 756902, fax: +44 (0) 1243 786300 or email: nicky@summersdale.com.
Disclaimer
Every effort has been made to ensure that the information in this book is accurate and current at the time of publication. The author and the publisher cannot accept responsibility for any misuse or misunderstanding of any information contained herein, or any loss, damage or injury, be it health, financial or otherwise, suffered by any individual or group acting upon or relying on information contained herein. None of the opinions or suggestions in this book are intended to replace medical opinion. If you have concerns about your health, please seek professional advice.
In memory of my grandfather, who taught me so much
And for my nephew, Simon, for his work with Alzheimer’s Society
Acknowledgements
I would like to thank Isabel Atherton, my wonderful agent at Creative Authors, for helping to bring another book in this series to fruition. Thanks also to Claire Plimmer at Summersdale who commissioned this and the previous titles, and to Stephen Brownlee who has guided it through the various stages towards publication. Thanks to my editor, Jennifer Barclay. It was good to work with her again and I am grateful for the many helpful suggestions she made. Thanks also to Julian Beecroft, my copy editor, who helped to smooth out the manuscript, and Vicki McKay, my proofreader. It has been a great pleasure to work with them all.
Finally, a huge thank you to Professor Graham Stokes for taking the time from his busy schedule to write the foreword to this book. I particularly valued his opinion as a clinician and academic working in the field of dementia.
Keith Souter
Contents
Cover
Title Page
Copyright Page
Dedication
Acknowledgements
Foreword
by Professor Graham Stokes, Global Director of Dementia Care, Bupa
Introduction
PART ONE: UNDERSTANDING DEMENTIA
Living well with dementia
Chapter 1: So what is dementia?
A brief history of dementia
Dementia around the world
The UK situation
Early onset dementia
Future prospects
Chapter 2: Understand the brain
The nervous system
The nineteenth century – major advances
The all-important nerve cells
White matter and grey matter
Neurotransmitters
The parts of the brain
The cranial nerves
The spinal nerves
The autonomic nervous system
The mind and the brain
Chapter 3: What happens in dementia
The ageing brain
Common symptoms of dementia
Getting a diagnosis
What happens to the brain in dementia?
The stages of dementia
The different types of dementia
Chapter 4: Alzheimer’s disease
The ‘disease of forgetfulness’ – the first case described by Dr Alzheimer
Atrophy
Neurofibrillary tangles
Senile plaques
Fewer neurotransmitters
Some theories about the cause of Alzheimer’s disease
The main features of Alzheimer’s disease
Four different presentations of Alzheimer’s disease
Posterior cortical atrophy
Hippocampal-sparing Alzheimer’s disease
Chapter 5: Vascular dementia
The blood supply of the brain
Stroke
The different types of vascular dementia
Risk factors for vascular dementia
The main features of vascular dementia
The treatment of vascular dementia
Chapter 6: Dementia with Lewy bodies and Parkinson’s disease dementia
Dementia with Lewy bodies, DLB
Parkinson’s disease dementia, PDD
Lewy bodies and the Lewy body spectrum
Symptoms in dementia with Lewy bodies
Dementia with Lewy bodies and Parkinson’s disease dementia – the differences
General treatment in dementia with Lewy bodies
Medical treatment of dementia with Lewy bodies
Treatment of Parkinson’s disease dementia
Chapter 7: Fronto-temporal dementia and other dementias
Fronto-temporal dementia, FTD
Other, rarer types of dementia
Chapter 8: Depression, delirium and mild cognitive impairment – things that can be confused with dementia
Depression
Delirium
Hypothyroidism
B12 deficiency
Parkinson's disease
Deafness
Brain tumour
Charles Bonnet syndrome
Mild cognitive impaiment, MCI
PART TWO: DEALING WITH DEMENTIA
Use it or lose it
Chapter 9: Getting the ball rolling – diagnosis
Getting a diagnosis
The memory clinic
The processes involved
The diagnosis
Continuing contact and support
Get a community care assessment
Chapter 10: So I have dementia
Talk about it
Normal emotions to have
Be proud of who you are
Coping with memory problems
Things you can do to help yourself
Maintain your independence but accept help
Get organised
Chapter 11: Caring for someone with dementia
You are not alone
Effective communication
Early stage care
Middle stage care
Late stage care
End of life
Becoming a carer
Chapter 12: Medical treatment
Cognitive enhancers
The treatment of vascular dementia
Drugs for other mental problems in dementia
Chapter 13: Care homes
Types of care home
When and how the decision is made
Choosing a care home suitable for the person with dementia
Chapter 14: Using the Life Cycle to help cope with dementia
The Life Cycle
The sphere of emotion
The sphere of the mind
The sphere of behaviour
The sphere of lifestyle
The sphere of body
Putting it all together
Chapter 15: What can you do to reduce your risk of dementia?
Risk factors for dementia
Four important factors that shrink the brain
Reduce your risk of dementia by being an optimist
Keep up your interests
Consider delaying retirement
Adopt good basic health habits
Get into a good sleep pattern
Eat fish
Finally, it is not all doom and gloom
Appendix
Glossary
Directory of useful addresses
References
Foreword
By Professor Graham Stokes
Global Director of Dementia Care, Bupa
Honorary Visiting Professor of Person-Centred Dementia Care, University of Bradford
Co-Chair, Dementia Action Alliance
In the United Kingdom the number of people with dementia is set to double over the next 35 years to reach nearly 1.75 million. Most will also be experiencing the ravages of advanced old age. There is no doubt this will exercise an unprecedented burden of responsibility on the NHS and caring services, yet this staggering increase in the numbers living with dementia, the most common cause of which is Alzheimer’s disease, is no longer solely a concern for health officials, doctors and social services. Rather, as dementia touches every family in the land, there is a need for society to become more dementia aware, to become more dementia friendly, and embrace a personal and civic responsibility to be informed about not simply the nature of dementia, but also how to understand what it means to live with a condition of the brain that progressively destroys the ability to remember, speak and reason, and what it takes to care well for someone living with a condition that eventually destroys self-awareness – an understanding that embraces the knowledge that for both those who care and those who need to be cared for there is rarely any true respite.
If it is possible for a book to explain the nature of dementia and brain function, address the experiences that comprise living and coping with dementia, and how to navigate the labyrinthine world of health and social care, this one does. Through fifteen informative, engaging and accessible chapters Keith Souter provides knowledge and insights that embrace not only the pathology of dementia but brings the need to live well with dementia to the fore. Each chapter contributes to the weaving of a tapestry that successfully integrates biology, person and care to give an overview of a journey with dementia from what can be done to reduce risk, to getting a diagnosis, to eventually sound advice regarding the choice of a care home. Complex information is rendered meaningful and summarised as ‘key points’ providing the reader with an excellent overview of the diseases that cause dementia as well as what is not dementia but may appear so, and of great importance ‘tips’ on not only how to survive with dementia but how to be a person who confronts and rises above the emotional and practical challenges that confront all those affected. Throughout, this guide resonates with the need to be person-centred in all that is planned and provided.
I am in no doubt that the subject of this book is of increasing and pressing importance. All involved in the support and care of people with dementia, all who know someone who appears muddled and absent-minded whether that is a partner, relative, friend or neighbour, as well as those who are or fear they may be living with the beginnings of dementia will benefit from investing their time in reading this guide.
We are motivated to understand how we can help people with dementia and their carers have fulfilling lifestyles that truly reveal life is worth living. We should be grateful for this book.
Introduction
One of the greatest fears that most people have is that they may lose their mental function and end their days slipping into dementia. Many of us will have had a relative with dementia and seen a gradual deterioration in their mental and physical health. The idea of losing control of one’s thoughts, memory and ability to communicate causes understandable anxiety.
Unfortunately, there is still a stigma about dementia. Inevitably, this makes people reluctant to talk about it, leading to a lot of ignorance on the subject. A result of this is that people who have dementia can feel isolated. Even worse, people who have memory problems or may be in the early stages of dementia can feel ashamed to have developed something that is stigmatised. This is something that we as a society have to work to overcome. The fact is, there is no shame at all in having dementia.
There is every need to keep people with dementia active and integrated into society. In this regard, being friends with people who have dementia, and having a supportive and caring attitude, can help them to deal with their condition.
Dementia is not a single condition, but an umbrella term used for a group of brain disorders that cause a deterioration of intellectual faculties such as memory, concentration and judgement. It is often accompanied by emotional disturbance and personality changes. The commonest form is Alzheimer’s disease, which accounts for about 60–70 per cent of cases, followed by vascular dementia, which makes up about 20 per cent. We shall consider these and the other types later in the book.
Dementia has been observed in all societies and cultures throughout history. The name comes from the Latin demens, which means ‘out of one’s mind or senses’, a bleak phrase that gives some idea why, in the past, people suffering from dementia were given so little help. They were left in the care of the family and, when the family could no longer deal with them, they might end up being admitted to a residential home or a psychiatric hospital. Treatment was often minimal, amounting to sedation with tranquillisers to keep them ‘manageable’.
Fortunately, today there is growing recognition that a person with dementia can continue to live well and enjoy life. Well-known people, such as the novelist Sir Terry Pratchett among many others, have done much to show that they can still be useful and contribute to society even after a diagnosis has been made.
The diagnosis can be frightening for the individual, with the potential to have devastating consequences for the most important relationships in someone’s life. Thus it is important to maintain the dignity of a person with dementia, to prevent them from simply being someone who receives care. Their uniqueness as an individual, their personal worth and their personal needs must always be of paramount importance. For this reason, a person-centred approach is what is needed.
The purpose of this book is to help the individual who may be experiencing memory problems, or who is concerned that they or a friend or relative might be developing dementia, by explaining the way the brain works and the various types of dementia, the tests that may lead to a diagnosis and the help that may be available. It also aims to dispel some of the myths that surround the condition. In addition, it will cover the treatments available and the strategies that can deal with the illness as it develops.
Part One
UNDERSTANDING DEMENTIA
Living well with dementia
In 2009 the UK government set out a National Dementia Strategy, called Living Well with Dementia.1 This recognised that although dementia is a progressive condition that gets worse over time, people who have the condition can still have a good quality of life for several years.
The strategy is aimed at people with dementia as well as carers, health professionals and anyone who is affected by dementia. That may mean friends or relatives of someone with dementia.
There are three key steps in this strategy:
• Ensure better knowledge and understanding about dementia
• Ensure early diagnosis, support and treatment of people with dementia, and support for their family and carers
• Develop services to meet changing needs.
All of this is important. As dementia is becoming increasingly common, we must be prepared as a society to improve the care people receive and to ensure that people are enabled to live well with the condition. It is important to offer early diagnosis so that whatever supports are needed can be given.
Chapter 1
So what is dementia?
The World Health Organization uses the definition given by the International Classification of Diseases.2
Dementia is a syndrome due to disease of the brain – usually of a chronic or progressive nature – in which there is disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. Consciousness is not clouded. The impairments of cognitive function are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behaviour, or motivation. This syndrome occurs in a large number of conditions primarily or secondarily affecting the brain.
The point about there being no impairment of consciousness is very important, since it can help to differentiate between dementia itself and potentially reversible conditions that may mimic the condition. This will be explained later.
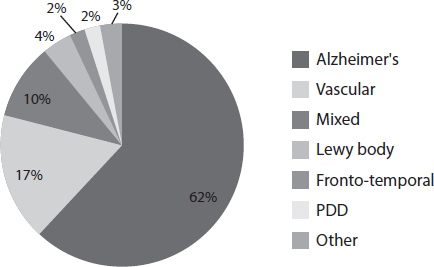
There are over 200 types of dementia, but the most common according to figures from Alzheimer’s Society are:
• Alzheimer’s disease: the commonest – accounts for 62 per cent of cases of dementia
• Vascular dementia: the second commonest – 17 per cent
• Mixed pattern – 10 per cent
• Dementia with Lewy bodies – 4 per cent. It has characteristics of both Alzheimer’s disease and Parkinson’s disease and also Parkinson’s disease dementia PDD
• Fronto-temporal dementia – 2 per cent
• Parkinson’s disease dementia PDD – 2 per cent
• Others including Creutzfeldt-Jakob disease, Korsakoff’s psychosis, and Huntington’s disease.
Causes of dementia in the UK
KEY POINT
Dementia is NOT a normal part of ageing.
A brief history of dementia
Dementia is not a new condition but has been recognised for centuries. It is instructive to consider how it has been regarded down the years and to see how we have gradually come to understand more about it. Thus we now realise that dementia is merely an umbrella label for a wide spectrum of brain disorders.
Ancient Egypt
The ancient Egyptians left us a great deal of information about their civilisation in tomb paintings and in the many papyri that have been discovered by archaeologists. In 1862, Edwin Smith, a young amateur Egyptologist and adventurer, purchased two papyri in Luxor, said to have been found between the legs of a mummy in the Theban necropolis. Both papyri dated to about 1550 BC, but were thought to be copies of far older texts. One is the oldest-known surgical text in the world, describing surgical instruments and techniques and discussing 48 cases of injuries, including head injuries. The other is a medical text outlining knowledge about medicine and the treatments used for a whole range of conditions.3
The Egyptians had hieroglyphics for the brain, the skull, the spinal fluid and the meninges, and the coverings of the brain, as well as for the other major organs. They knew that the brain was needed to control the movements of the body, and they recognised that injury to one side of the brain could result in paralysis of the opposite side of the body.
A beautiful and historically accurate description of ancient Egyptian surgery is given in the 1945 historical novel The Egyptian by the Finnish writer, Mika Waltari. The main character Sinuhe, who would become the royal physician to Pharaoh Akhenaten, is apprenticed to the ‘opener of heads’. He shows him how to examine a patient and diagnose where there may be a problem in the head from an assessment of the state of consciousness and the use of the limbs. He then shows him how to remove a piece of skull and replace it with a silver plate, which is bound with bandages while they await recovery.
Although the Egyptians had accumulated this knowledge they did not recognise the importance of the brain as the organ of thought. This is understandable, since emotions often seem to relate to the chest and to the beating of the heart. During the mummification process they preserved the heart and other organs, but the brain was removed by pulling it down through the nose and discarding it. It was not believed to be needed in the afterlife.
Nevertheless, they described the state of dementia. They believed that it was related to age, although it was not something that inevitably happened to everyone.
The ancient Greeks
Hippocrates, the father of medicine, described the condition that we can recognise as dementia in the fifth century BC. Although it had been observed before then, it was considered a disorder caused by demonic possession, as in those days so many conditions were thought to have a supernatural origin. Hippocrates was one of the first doctors to suggest that the brain was the seat of the mind. Furthermore, he differentiated between mania, melancholia and dementia. Essentially, he recognised that dementia was progressive and that it was very different from depression (melancholia) and other mental illnesses.
In the second century the Greek physician Claudius Galenus of Pergamum (AD 131–201), better known as Galen, performed several dissections on animals and accurately described many of the organs of the body. He described the function of the nerves, and examined the structures of the eyes, ears, larynx and reproductive organs. He taught that psychic gases and vital fluids called humours flowed through the body into the ventricles of the brain, thereby allowing for the development of mental functions. In his writings he also described age-related forgetfulness. This he attributed to weakening of the humours that flowed through the brain.
Aretaeus of Cappadocia at the end of the second century distinguished between acute and chronic conditions of the mind. Acute disorders, he said, were reversible and he called them delirium. Chronic disorders associated with loss of memory and other mental symptoms he called dementia. He said that these were irreversible. This, as we shall see in Chapter 8 (Depression, delirium and mild cognitive impairment – things that can be confused with dementia) was pretty accurate and accords with what we now know.4
The rise of anatomy
The early Christian Church banned the anatomical dissection of the body and it was not until the sixteenth century that further advances in knowledge about the brain were made. Andreas Vesalius (1514–1564) was a Flemish anatomist who demonstrated that Galen and other early anatomists had been incorrect in some of their conclusions. In 1543 he wrote the first anatomically accurate medical textbook, De Humani Corporis Fabrica (On the Fabric of the Human Body), complete with precise illustrations of the brain. He believed that the brain and nervous system were the seat of the mind and the emotions. Deterioration of the brain would result in diminished power of the mind.
One of King Charles I’s physicians was Dr Thomas Willis (1621–1675), an anatomist who was deeply interested in the blood supply of the body. He published several books in the 1660s, the most significant being a work about the brain. In it he described the circle of blood vessels at the base of the brain, which were formed from major arteries travelling up the front of the neck to join with ones from the back of the neck to produce an arterial circle which gave off branches to supply blood to the various areas of the brain. This is called the Circle of Willis.
In 1672 he described ‘dementia postapoplexy’, meaning dementia arising after patients had suffered from strokes, apoplexy being the old name for stroke. He was quite correct in his conclusion, since this is one of the causes of vascular dementia, which we will look at in Chapter 5 (Vascular dementia).
France and the father of psychiatry
French physician Philippe Pinel (1745–1826) is regarded as the father of modern psychiatry. It was the practice before then to treat patients with mental illness in asylums and with widespread use of restraints. When he became the medical superintendent of the Hospice de la Salpêtrière in Paris, he ordered that the shackles should all be struck off the patients and he introduced humane treatments. Not only that but he began a systematic classification of mental illness and in particular started using the term ‘dementia’. Although there is record of the word being used earlier, this was the first instance of its use as a medical diagnosis.
At about the same time another French physician, Jean-Étienne Esquirol (1772–1840), wrote a book called Des Maladies Mentales in which he listed a range of causes of dementia, including those we would recognise today, such as repeated head injuries and mercury poisoning, but also fanciful causes like haemorrhoids, masturbation and domestic problems. Nevertheless, it was an attempt to search for reasons why people might have developed the condition.
Pathology and Alzheimer’s disease
In the nineteenth century, post-mortem anatomical examination became an accepted part of medical science. It allowed doctors to examine organs and correlate pathological changes with signs and symptoms experienced by patients in life, in order to build up a real picture of what happens in disease.
Arnold Pick, a Czech physician (1851–1924), was professor of neurology and psychiatry at Prague. In 1892 he described a condition in which there is atrophy of the frontal and temporal lobes of the brain (see Chapter 2), which resulted in senile dementia. It became known as Pick’s lobar atrophy, one of the rarer types of dementia. He went on to write a book on neuropathology.
Emil Kraepelin (1856–1926) was a German psychiatrist, now regarded as the founder of scientific psychiatry. He believed that most mental disorders had a biological basis and that this could be defined in pathological changes that could be found in the brain. He did important work with many of the severe mental disorders, including bipolar disorder and schizophrenia.
A colleague of his was Alois Alzheimer (1864–1915), a German psychiatrist and neuropathologist. When he was working in the Frankfurt Asylum in 1901, he observed a 51-year-old female patient with significant memory and behavioural problems. When she died he examined her brain using staining techniques. These showed the presence of amyloid plaques and neurofibrillary tangles. He thereby described for the first time the pathological signs of dementia (see Chapter 4, Alzheimer’s disease).
Kraepelin wrote a textbook subsequent to Alzheimer’s discovery in which he referred to two types of dementia: a presenile variant which he called Alzheimer’s disease and a senile type. This differentiation into two types was maintained in the textbooks for decades, until it was realised that they were not two separate conditions and that age was not a valid differentiator; the pathological changes were the same. Nevertheless, as we shall see later, it is important to consider the needs of what we now call early-onset dementia.
Otto Binswanger (1852–1929) was a Swiss psychiatrist and neurologist who also did extensive work on the brain. In 1894 he described a condition which he called ‘encephalitis subcorticalis chronica progressiva’, which was associated with memory problems and intellectual difficulties. It is one of the rare forms of dementia and is due to small blood vessel damage to the white matter of the brain. Today we know it as subcortical dementia or Binswanger’s disease (see Chapter 5, Vascular dementia).
Dementia around the world
Dementia is not something that people like to think about – not just individuals, but society as a whole. It is, in fact, a colossal problem throughout the world, as the following figures show:
KEY POINTS
In 2012 the World Health Organisation produced a report, Dementia – a Public Health Priority. It set out a fairly stark picture, suggesting that the world faces a dementia time bomb. It acknowledges that people are living longer and that there have been significant improvements in health, especially through vaccination and better management of infectious diseases. On the other hand, the incidence of non-communicable disease, including dementia, is increasing. In part the rise in the number of cases of dementia is because of this increase in life expectancy.
The report suggests that because people go on living for many years after the diagnosis of dementia, it is imperative that adequate support should be available for people living with the disease.
The UK situation
The UK has a population of over 63 million, the third largest in the European Union.5 According to Alzheimer’s Society, in 2013 there were more than 800,000 people with dementia in the UK, comprising:
• More than 665,000 in England
• More than 86,000 in Scotland
• More than 18,000 in Northern Ireland
• More than 44,000 in Wales.
There are 163,000 new cases of dementia in the UK every year.
In the UK about 25 million people, or 42 per cent of the population, know a close friend or relative with dementia (Alzheimer’s Research UK). Dementia is commoner in older people, but it occurs in all ages:
• One in 1,400 people aged 40–64 years have dementia.
• One in 100 people aged 65–69 years have dementia.
• One in 25 people aged 70–79 years have dementia.
• One in 6 people aged 80 years and over have dementia.
In 2013 dementia was recorded as the 3rd most common cause of death in the UK, after heart disease and stroke.
Early onset dementia
Early onset dementia is when dementia occurs in people under the age of 65 years. It may also be called dementia in younger people or young-age dementia. Currently, there are more than 44,000 people in the UK with early onset dementia.
The symptoms experienced can be exactly the same as with any other form of the condition, but the needs of the person with early onset dementia may be different.
For example, a person with early onset dementia may:
• Be in employment
• Have a partner who is in employment
• Have children dependent on him or her
• Have parents who may be dependent on him or her
• Have financial commitments.
The cause of early onset dementia can be the same as with dementia affecting people over the age of 65 years. Alzheimer’s disease is still the commonest cause, but it makes up only a third of cases, whereas in older people it makes up two thirds. Vascular dementia is the next most common, causing 20 per cent of cases. However, fronto-temporal dementia causes 12 per cent of early onset dementia compared to only 2 per cent of cases in older people.
Diagnosis in this group is often delayed, partly because it is often not considered at a younger age and because the person may not ask for help or even realise that they have a problem. Once dementia is suspected, the GP will usually refer their patient to a neurologist rather than to a psychiatrist, because of the need to pinpoint the diagnosis.
KEY POINTS
Future prospects
The World Health Organisation estimates that the number of people around the world living with dementia will double by 2030 and triple by 2050. There is one new case of dementia every four seconds.
According to Alzheimer’s Society the number of people with dementia in the UK will rise dramatically as the population ages. It is estimated that whereas in 2014 there were 800,000 people with dementia in the UK, this figure will rise to one million by 2021 and to 1.7 million by 2051.
FAMOUS PEOPLE WHO HAVE HAD OR HAVE DEMENTIA
There is no shame in having dementia. Everyone can leave their own mark in life and this should be celebrated. We should strive to help every person with dementia to live well. All of these people had or have dementia yet all have contributed to the world:
Chapter 2
Understand the brain
The brain is the most important organ in the body. It controls the way that you move, and it perceives all of the information that is transmitted to it from the sense organs of touch, vision, hearing, smell and taste. It is also where you perceive pain.
You might say that the brain is the essence of the individual, since it is where all of the thinking and emotions seem to take place. That is, the brain seems to be the seat of the mind, an idea widely debated by philosophers and scientists almost since the beginning of human consciousness. We will come back to this later in the chapter, since it is important in our understanding of the brain and our consideration of dementia.
Figure 1
BASIC BRAIN FACTS:
The nervous system
The nervous system is the body’s main communication system. It is customary to consider it as having two parts, the central nervous system, consisting of the brain and spinal cord, and the peripheral nervous system, consisting of the nerves to the various parts of the body. In addition, there is the autonomic nervous system, which controls the function of the internal organs.
The nervous system controls every aspect of your life, ranging from the involuntary functions like breathing to the voluntary functions of moving. The brain, of course, is the great computer of the body where all the information from sensory nerves is transmitted and where thoughts and decisions are made, and it is from there that nerve impulses are transmitted down motor nerves to make muscles move.
The nineteenth century – major advances
The Victorian era saw an explosion in knowledge in all areas of science, including medicine. In regard to the brain there were three major discoveries.
The speech centre
In the mid-nineteenth century the French surgeon and anthropologist Pierre Paul Broca (1824–1880) discovered that the left hemisphere of the brain was dominant in speech production. He localised this to a very specific area in the frontal lobe of the dominant hemisphere. It was named after him as Broca’s area.
Language comprehension