Title Page
Copyright Page
Foreword
Preface
Acknowledgements
Chapter 1 The Goals and Clinical Outcomes of Non-Surgical Treatment
Aims
Outcome
The Periodontal Pocket – A Pathological Environment
The Aims of Non-Surgical Treatment
Elimination of Calculus
The Concept of Full-Mouth Disinfection
Healing Following Periodontal Treatment
Clinical Outcomes Following Non-Surgical Treatment
Hygiene versus instrumentation phases
The Badersten studies
An evidence base for non-surgical treatment
Summary
Conclusions of Clinical Importance
Further Reading
Chapter 2 Hygiene Phase Therapy
Aims
Outcome
Plaque Control Programmes
Mechanical plaque control
Manual Toothbrushes
Powered Toothbrushes
Toothpastes
Toothbrushing techniques
Bass Technique
The Charters’ Method
Interproximal Cleaning Aids
Dental Floss and Tape
Superfloss
Interspace Brushes (Fig 2-6)
Interdental Brushes (Fig 2-7)
Woodsticks (Fig 2-8)
Chemical Plaque Control (Fig 2-9)
Cationic agents
Quaternary ammonium compounds (QACs)
Phenols
Listerine™
Triclosan™
Plax™
Sanguinarine
Heavy metal salts
Zinc salts
Tin salts
Enzymes
Lactoperoxidase-hypothiocyanite
Key Points of Clinical Importance
Further Reading
Chapter 3 Instruments and Instrumentation
Aim
Outcome
Introduction
Hand Instruments
Chisel Scaler or Push Scaler (Guy’s G1 or G2, Cushings or Watch-Spring)
Trihedral Scalers (H6, H7, G3, G4, J1 and H5)
Periodontal Hoes
Periodontal Files (Hirschfeld 3/7, 5/11 and 9/10)
Curettes
Universal Curettes (Columbia 2R/2L; Columbia 13/14; Langers 1/2; Langers 5/6, and Langers)
Area-specific curettes/site specific curettes
Recommended Protocol for Root Surface Instrumentation (RSI)
Mechanised Instruments
Ultrasonic Units
Magnetostrictive Units
Inserts for magnetostrictive units
Piezoelectric Ultrasonic Units
Inserts for piezoelectric units
Sonic Handpieces
Inserts for sonic handpieces
Air-Abrasive Systems
Ultrasonic Techniques
Periodontal Explorer
Repetitive Strain Injury
Conclusions of Clinical Importance
Further Reading
Chapter 4 Managing Systemic Risk Factors
Aim
Outcome
Definitions
Risk Factor Identification
Genetic Risk Factors for Periodontitis
Genetic Susceptibility Testing
What do genetic test results mean, and what is their impact on the patient?
Environmental Risk Factors for Periodontitis
Drugs Associated With Gingival Overgrowth
HIV Disease
Behavioural Risk Factors for Periodontitis
Smoking
Life-style Risk Factors for Periodontitis
Stress
Metabolic Risk Factors for Periodontitis
Diabetes Mellitus
Other Systemic Risk Factors for Periodontitis
Conclusions of Clinical Importance
Further Reading
Chapter 5 Managing Local Risk Factors
Aim
Outcome
Definitions
Trauma from occlusion
Traumatic Incisor Relationships
Occlusal Interferences
Anatomical Risk Factors
Furcation Involvement
Enamel Pearls
Cervical Enamel Projections
Root Morphology
Gingival Recession
Furcation Ridges
Dental Anatomy and Tooth-Arch Relationships
Iatrogenic Risk Factors
Overhanging Restorations
Poorly Designed Partial Dentures
Orthodontic Appliances
Defective Crown Margins
Defective Bridge Pontics
Conclusions of Clinical Importance
Further Reading
Chapter 6 Adjunctive Treatments
Aim
Outcome
Definitions
Systemic Adjunctive Treatments
Systemic Antibiotics
Antibiotics and Specific Periodontal Conditions
Chronic Periodontitis
Aggressive Periodontitis
Refractory Periodontitis
Acute Periodontal Abscess
Necrotising Ulcerative Gingivitis and Periodontitis
Systemic Antibiotics – Summary
Host Modulatory Therapy
Non-Steroidal Anti-Inflammatory Drugs
Subantimicrobial Dose Doxycycline
Bisphosphonates
Local delivery adjunctive treatments
Tetracycline Fibres
Minocycline Gel
Metronidazole Gel
Chlorhexidine Chip
Doxycycline Polymer
Which local delivery product to use, and when?
Adverse reactions and local drug delivery
Monotherapy or adjunctive use of local delivery systems?
Key points of clinical importance
Further Reading
Chapter 7 Supportive Periodontal Care
Aims
Outcome
Definitions
The Rationale for Supportive Periodontal Care
The Goals of Supportive Periodontal Care
Components of Supportive Periodontal Care
Medical, Dental and Social Histories
Clinical Examination and Updating Records
Radiographic Examination
Communication
Reinforcement of Plaque Control
Supragingival Prophylaxis and Subgingival Instrumentation
The Need for Further Treatment
Re-instrumentation of the Roots
Adjunctive Antimicrobials
Commencement of the Supportive Periodontal Care Phase
Frequency of Visits for Supportive Periodontal Care
Managing Risk Factors During Supportive Periodontal Care
Compliance with Supportive Periodontal Care
Ways to improve patient compliance
Conclusions of Clinical Importance
Further Reading
Quintessentials of Dental Practice – 16
Periodontology – 3
British Library Cataloguing in Publication Data
Heasman, Peter A.
Successful periodontal therapy : a non-surgical approach. - (Quintessentials of dental practice. Periodontology; 16. Periodontology; 3)
1. Periodontal disease - Treatment
I.Title II.Preshaw, Philip III.Robertson, Pauline
617.6′3206
ISBN 1850973156
Copyright © 2004 Quintessence Publishing Co. Ltd., London
Figs 4-1, 4-3, 4-5 by Laura Andrew
All rights reserved. This book or any part thereof may not be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, or otherwise, without the written permission of the publisher.
ISBN 1-85097-315-6
Successful periodontal therapy is, for many, fundamental to the goal of teeth for life. With a state-of-the-art non-surgical approach to periodontal therapy, success is dependent on a plethora of interrelated factors and influences, including the complexity of the disease process, predisposing risk factors, diagnostic skills and techniques, patient management and motivation, knowledge of modern instrumentation, techniques and adjunctive treatments, not to forget clinical acumen both during active treatment and the equally critical long-term supportive periodontal care. Can all of this be covered effectively in a slim, easy-to-read book? Yes, it can: the authors of Volume 16, Periodontology 3 in the Quintessentials of Dental Practice Series have achieved this feat, with plenty extra packed in by way of a bonus.
It is proving to be a great learning experience being Editor-in-Chief of the Quintessentials of Dental Practice Series, the present book having added greatly to my new enlightenment. Dental students, trainee hygienists and therapists and practitioners of all ages, not to forget everyone’s patients, will benefit enormously from this timely contribution to the existing literature. I hope you enjoy and learn from this excellent book as much as I did.
Nairn Wilson
Editor-in-Chief
This text is the third of five books that aim to provide the general dental practitioner with an illustrated practical and contemporary guide to the management of patients with gingival and periodontal diseases. This book is entitled Successful Periodontal Therapy: A Non-Surgical Approach. Initially it presents the reader with recognised goals and objectives of non-surgical treatment. Subsequent chapters cover the clinical protocols and methods for achieving these goals: hygiene phase; scaling and root surface instrumentation; the instruments used for scaling and root surface debridement; managing common and well-established risk-factors; and the use of treatments that are considered to be adjunctive to conventional methods of scaling and root surface instrumentation. The final chapter reviews the importance of supportive periodontal care, which is highly relevant for general dental practitioners, for both those patients that they have treated in the primary care setting and those who may have received their non-surgical management by a specialist or in a hospital environment.
It is hoped that having read this book on periodontal therapy the reader will be able to:
understand the healing events that follow non-surgical treatment
realise the limitations of non-surgical treatment
have knowledge of the range of mechanical and chemical products that are available to improve personal plaque control
be aware of the range of instruments that are available for removing tooth deposits
understand the importance of identifying and managing systemic and local risk factors for periodontal diseases
understand the importance of identifying and managing local anatomical and iatrogenic factors that may predispose to periodontal disease
be aware of systemic and locally-delivered adjunctive treatments that are available and know how to reach informed decisions regarding the most appropriate product for any specific clinical situation
understand the goals of supportive periodontal care and how they might be achieved
appreciate the need for patient compliance and understand how poor patient compliance might be identified and improved.
Peter Heasman
Philip Preshaw
Pauline Robertson
Iain Chapple
The authors would like to acknowledge with sincere thanks the following people: Janet Howarth of the Department of Dental Photography at Newcastle Dental Hospital for her photographic expertise; Dr David Jacobs for Fig 5-1; Dr Shakil Shahdad for Figs 5-2 and 5-3; Dr Robert Wassell for Fig 5-5; Dr Dean Barker for Figs 5-8, 5-9 and 5-10; Dentsply UK for Figs 3-4, 3-6, 3-7, 3-9, 3-10 and 3-14. We are grateful also to Professor Iain Chapple for Figs 3-15, 5-7 and 5-11 and Mrs Suzanne Noble for use of Figs 3-16, 3-17 and 3-18. Permission has been granted to reproduce the following: Fig 2-4 (from Heasman, Millett, Chapple. The Periodontium and Orthodontics in Health and Disease. Oxford; Oxford University Press: 1996); Fig 5-5 (from Barnes, Walls. Gerodontology. Oxford; Wright: 1994); Fig 5-20 (from Heasman, Preshaw, Smith. Periodontology Colour Guide. London; Churchill Livingstone: 1997). Thanks to Iain Chapple and Damien Walmsley for the cover photograph and to George Warman Publications, publishers of Dental Update, for permission to reprint part of this image.
Professor Heasman would like to acknowledge the support of Lynne, Sophie and Christopher, during the preparation of this book. Dr Preshaw would like to thank his wife, Sarah, for her help and support. Pauline Robertson would like to acknowledge the support of her husband, Brian, and family.
This chapter aims to outline the goals of non-surgical periodontal treatment and to provide an overview of the clinical outcomes that are expected following treatment.
After reading this chapter the practitioner should have an understanding of:
the healing events that follow non-surgical treatment
the magnitude of the clinical changes and outcomes expected following the hygiene (or initial) and instrumentation (or corrective) phases
the limitations of non-surgical treatment.
A periodontal pocket is a pathologically deepened gingival crevice. The lateral and apical boundaries of the pocket are the ulcerated epithelial lining of the pocket wall and the junctional epithelium respectively. The remaining “wall” of the defect comprises the diseased root surface – the “target” for periodontal treatment.
The diseased root surface is contaminated with subgingival calculus deposits and a layer of dental plaque, which contains the periodontal pathogens that constantly challenge and compromise the host’s defence mechanisms. Dental plaque is now regarded as a biofilm, which essentially is an organised community of bacteria that forms on a non-shedding surface such as a tooth. Bacteria attach to the tooth and produce a matrix of extracellular polymers to help bind them together. Microcolonies form and new species join the biofilm which then contains diverse species and metabolic states. Gingival crevicular fluid (GCF) flows through the many channels in the aggregation to provide nutrients and to remove some of the waste products. The biofilm is viable and bacteria can proliferate to establish new colonies on other parts of the root surface.
The majority of bacteria in an established biofilm are recognised, anaerobic organisms with cell walls containing powerful lipopolysaccharide (LPS) based endotoxins. Studies have shown that the vast majority of LPS is only loosely bound to, or associated with, the root surfaces although a small percentage of the total LPS may cause subsurface contamination, in particular at sites of root surface irregularities, root grooves or resorption lacunae. Subgingival calculus on the root surface may also be contaminated with LPS. Diagrammatic representations of a diseased root surface are shown in Fig 1-1.
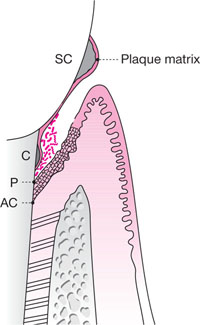
Fig 1-1 Diagrammatic representation of a periodontal pocket for a patient with chronic periodontitis. The pocket epithelium, which
is ulcerated, has migrated down on to the root surface. Calculus deposits are present both supra- and subgingivally and these
deposits are covered with a layer of plaque. The subgingival plaque may also be regarded as a biofilm with a complex population
of loosely adherent microoganisms on its surface.
SC, supragingival calculus
C, subgingival calculus
P, the most apical extent of the periodontal pocket
AC, the most apical cell of the junctional epithelium
The overall aim of non-surgical treatment is to create an environment that is biologically compatible with healing of the periodontal tissues. This is most likely to be achieved by:
decontamination by removing LPS/endotoxins from the root surface
disrupting and eliminating the biofilm from the root surface
removing the bulk of subgingival calculus from the root surface.
Laboratory studies have shown that a gentle stream of water can remove about 39% of the LPS whilst brushing the root surface eliminates a further 60%. This suggests that the hygiene phase of non-surgical treatment may be instrumental in disrupting the biofilm and eliminating up to 99% of endotoxins in the pocket. Such a hypothesis of course makes the assumption that the patient is able to access the entire depth of the pocket during cleaning. This is seldom achieved for pockets that are greater than 5mm in depth. Indeed, the deeper the pocket, the more residual, undisturbed biofilm is likely to remain.
The need for professional intervention is, therefore, crucial and this includes root surface instrumentation, a term which is used in preference to root planing. Root surface instrumentation describes the procedure that is necessary to eliminate endotoxins, disrupt the biofilm and, when present, remove subgingival calculus from the root surface (also called root surface debridement). Root surfaces that have no detectable subgingival calculus may be instrumented by passing an instrument such as an ultrasonic scaler lightly over the surface. This will remove the loosely associated toxins and the majority of the outermost, necrotic cementum on the root surface (Fig 1-2). Research shows that the most effective use of ultrasonic instruments involves multiple light passes of the instrument over the root surface. The presence of tenacious, subgingival calculus will, however, necessitate the use of greater pressure to the root, although the belief that the root surface has to be meticulously “planed” until it is hard and smooth is now largely outdated.
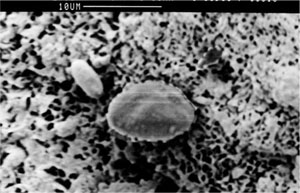
Fig 1-2 Scanning electron microscope view of a periodontally involved root surface showing porous and necrotic cementum.
Calculus is not the cause of periodontal disease, but may be regarded as a contributory factor, for several reasons including:
all calculus has a coating layer of dental plaque
supragingival calculus impedes toothbrushing and interdental cleaning
subgingival calculus may act as both a barrier to subgingival cleaning and a focus for the colonization of bacteria during the first stage in the formation of a biofilm
subgingival calculus may absorb bacterial endotoxins
supra- and subgingival calculus may impede the passage of periodontal probes, thereby falsifying borderline probing depth measures.
For these reasons, it is important to try to remove as much of the calculus as possible, although some residual, isolated deposits of subgingival calculus are likely to be compatible with periodontal healing. This observation is consistent with studies that have shown that even under optimal conditions of access during periodontal surgery absolutely calculus-free root surfaces following root surface instrumentation are hardly ever achieved. With the understanding that pockets with probing depths of >5mm are exceptionally difficult to render plaque and calculus free, it is almost certain that residual deposits are more likely to be the rule rather than the exception with a non-surgical approach.
The importance of eliminating the biofilm and bacteria that have freedom of movement around the oral cavity, and are the cause of periodontal infections and re-infections, has been recognised by the introduction of full-mouth disinfection as a novel treatment strategy for periodontal diseases. Full-mouth disinfection involves the conventional removal of root surface deposits, usually over two visits within 24 hours of one another. Instruction in oral hygiene procedures is also given at one or both visits. This treatment recognises, however, that many of the potent pathogens, such as Porphyromonas gingivalis and Actinobacillus actinomycetemcomitans, are also commonly found at non-periodontal sites such as on the dorsum of the tongue, on the oral mucosa, in saliva, or on the mucosal surface of the tonsils. Re-infection of treated pockets is, therefore, likely unless an attempt is made to eliminate the organisms from all of these niches and as quickly as possible. The fewer the number of visits, the less chance there is for re-infection from (as yet) untreated sites.
Different preparations of chlorhexidine gluconate have also been used in an attempt to achieve adjunctive disinfection immediately after the completion of root surface instrumentation (Table 1-1). There is little evidence, however, to support the clinical value of the adjunctive use of chlorhexidine over mechanical instrumentation alone during full-mouth disinfection.
| Preparation | Application |
| 1% gel | Brushing the dorsum of the tongue for 1 minute |
| 0.2% mouth rinse | Full-mouth rinse for 1 minute |
| 0.2% spray | Applied to the tonsil region |
| 1% gel | Repeated (x 3) subgingival irrigation over a 10-minute period |
| 0.2% mouth rinse | Twice-daily rinse for 1 minute at home for 2 months |
| 0.2% spray | Twice-daily application to tonsil region for 2 months |
One of the principal signs of a healing pocket is the reduction in probing depth that follows treatment. This reduction is largely a result of the resolution of gingival inflammation leading to shrinkage of the gingival tissues and the formation of a new, long junctional epithelium (Fig 1-3).
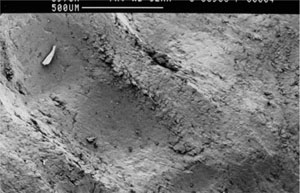
Fig 1-3 The root surface shown in Fig 1-2 has been instrumented using light application of an ultrasonic scaler. The root surface is now relatively smooth, although there are noticeable indentations as a result of the instrumentation.